
Saadiya Aziz Karim ( Departments of Obstetrics and Gynaecology, The Aga Khan University Medical Centre, Stadium Road, Karachi. )
Ikram Bakhtawar ( Departments of Obstetrics and Gynaecology, The Aga Khan University Medical Centre, Stadium Road, Karachi. )
Adnan T.Butta ( Departments of Obstetrics and Gynaecology, The Aga Khan University Medical Centre, Stadium Road, Karachi. )
Majid Jalil ( Departments of Obstetrics and Gynaecology, The Aga Khan University Medical Centre, Stadium Road, Karachi. )
February 1998, Volume 48, Issue 2
Original Article
Abstract
The effects of vaginal bleeding during first and second trimester on pregnancy outcomes was assessed in a hospital-based population of 268 non-diabetic women. The group of non-bleeders comprised 173 females whereas, there were 71 females with first and 24 with second trimester bleeding. Fetal loss (abortion) occurred in 34% of first trimester and 25% of second trimester bleeders. Low birth weight and preterm delivery were significantly associated with second trimester haemorrhage. The results suggest that first and second trimester vaginal bleeding correlates with adverse infant outcomes (JPMA 48:40, 1998).
Introduction
Vaginal bleeding is a common occurrence during pregnancy. Some degree of vaginal bleeding during the first trimester occurs in approximately 25% of pregnancies. Previous studies have shown a high rate of fetal loss and adverse infant outcomes like prematurity. Intrauterine Growth Retardation (IUGR). Still birth and neonatal death (NND) in pregnancies complicated by vaginal bleeding1-9. Such data about the Pakistani population is not available. In this study the association between vaginal bleeding in the first and second trimester and pregnancy outcome was assessed in a hospital based group of women. The outcomes considered included low birth weight (LBW). prematurity and term low birth weight.
Patients and Methods
To look at the effects of vaginal bleeding in early pregnancy on its outcome, a retrospective case control study was conducted at the Aga Khan University Medical Centre from January 1988 to December 1992. The information was gathered from the medical records review. The study group comprised 268 women. It was divided into cases and controls depending on the presence or absence of vaginal bleeding in pregnancy. The cases included 71 women with first and 24 with second trimester vaginal bleeding. Most of these women presented as cases of vaginal bleeding in early pregnancy either in the emergency or the obstetric clinics. The control group consisted of 173 women where the pregnancy was not complicated by vaginal bleeding. These were picked by systematic random sampling from the “Booking” obstetric clinic in the same time frame as the study. Pregnancies complicated by diabetes, placenta previa, hypertension in pregnancy and abruptio placenta were excluded. The risk of the following adverse outcome was evaluated. Low birth weight (both preterm and small-for- gestational age babies less than 2500 gms), preterm birth (before 37 completed gestational weeks) and term LBW (gestational duration 37 or more weeks but birth weight less than 2500 gms). The distribution of maternal socio-demographic characteristics and medical and reproductive histories were examined within the categories of women studied. The Chi square test was applied to assess the association and degree of significance of bleeding in pregnancy with adverse infant outcomes.
Results
The number of women who never bled during pregnancy was 173. Seventy one had first trimester and 24 had second trimesterbleeding. Approximately 75% of the vaginal bleeding was limited to the first and 25% to the second trimester. Only two women had bled twice, but both the episodes were limited to the first trimester.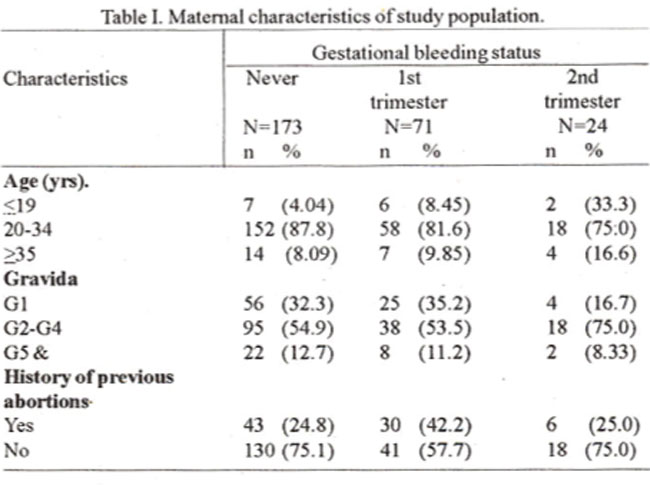
Table I lists selected maternal characteristics according to gestational bleeding status. Fetal loss (abortion) was observed in 4 out of 173 (2%) non-bleeders and in24 out of 71 (34%)firsttrimester bleeders and 6 out of 24 (25%) second trimester bleeders. “Non-bleeders” who subsequently aborted were distinguished from “Bleeders” by the fact that fetal demise (missed abortion) was discovered on routine ultrasound and there was no bleeding whereas the “Bleeders” presented with vaginal bleeding. Considering the associationoflowbirthweightwith first and second trimester vaginal bleeding, in the control group, 15 out of 160(9%) had birth weight <2.5 Kg, whereas, 8 outof42 (2 1%) first trimesterbleeders and 5 outof 15(33%) second trimester bleeders and birth weight _2.5 kg. The association of 2nd trimester bleeding with low birth weight is highly significant (X2 7.8, Th=0.005).
Pretermdeliveiy occurred in 12 outpf 169 controls (7%) and in 7 out of 47 first trimesterbleeders (15%) and 6 out of 18 second trimester bleeders (3 3%). The association between second trimester loss and preterm labour is highly significant (X2 12.9, P<0.001) (Table II).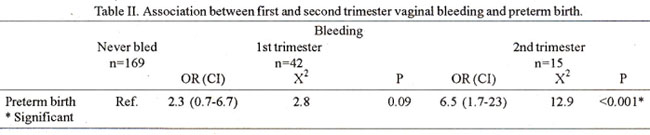
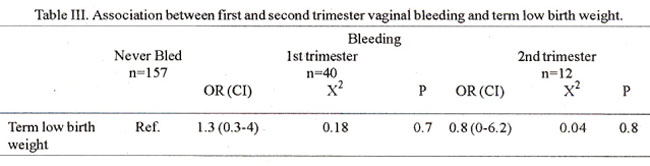
Table III shows that them is no statistically significant association between bleeding in the first two trimesters of pregnancy and low birth weight at term in this analysis. Ten percent of controls had low term birth weight, whereas, 12% of first trimester bleeders and 8% of second triemester bleeders had low birth weight at term. Intrauterine death was observed at term in one case of 1st trimester vaginal bleeding. She did not have any other complication during the course of her pregnancy and the cause of the fetal death remained undetermined.
Discussion
This study suggests that first and second trimester vaginal bleeding are important predictors of adverse infant outcomes. Both first and second trimester bleeding were associated with high early fetal loss (abortion). There was a statistically significant association between second trimester bleeding and low birth weight and preterm labour. Similar findings were reported by other workers10. This suggests that bleeding prolonged into the second trimester is likely to affect fetal outcome adversely. That limited to the first trimester may either end in abortion or (if not severe) may not affect fetal health unduly as enough recoveiy time is available. The infant outcomes studied here - preterm birth and low birth weight have been chosen because of their relevance with regard to infant morbidity and mortality11,12. The study design (retrospective, case control) has its limitations, as it involved review of the medical records. Some cases had to be dropped because of lack of data. This accounts for the variation in the number of women in the categories of infant outcomes studied. Strobino .and Silverman have linked frequency of low birth weight and preterm birth with the severity of maternal haemorrhage. This was not possible here as the patients could not be questioned directly regarding the amount of blood loss. It is suggested that a prospective multicentre study withalargerstudy populationbe carried out to substantiate the results of this preliminaiy analysis. This is particularly relevant in Pakistan where epidemiological data relating vaginal bleeding and pregnancy outcome is not available.
Acknowledgements
The authors are grateful to Mr. Javed Iqbal Qureshi, Secretary for assistance in preparation of manuscript.
References
1. Strobino, B. and Pantel - Silverman, J. Gestational vaginal bleeding and pregnancy outcome. Am.J. Epidemiol., 1989;129:806- 15.
2. Strobino, B. and Pantel-Silverman, J. First trimester vaginal bleeding and the loss of chromosomally normal and abnormal conceptiona. Am. J. Obstet. Gynaecol., 1987;157:1150-4.
3. Berkowitz, G.S.. Harlap, S., Beck, G.J. et al. Early geatational bleeding and pregnancy outcome: A multivariate analysis. Int. J. Epidemiol., 1983;12:16573.
4. Peckham, C.H. Uterine bleeding during pregnancy when not followed by immediate termination ofpregnancy. Obstet. Gynaecol., 1970;35 :937-41.
5. South, J. and Neldert, J. The effect ofvaginal bleeding in early pregnancy on the infant bom after the 28th week of pregnancy. J. Obatet. Gynecol. (Br. Commonw)., 1973;80:236-41.
6. Hertz, J.B. and Heiaterberg, L. The outcome of pregnancy after threatened abortion. ActaObatet. Gynecol. Scand., 1985;64:151-6.
7. Evans, J.H. and Beischer, N.A. The prognosis of threatened abortion. Mcd. J. Aust., 1970;2: 165-8.
8. Funderburk, S.J., Guthrie, D. and Meldrum, D. Outcomes of pregnancies complicated by early vaginal bleeding. Br. J. Obstet. Gynecol., 1980;87:100-5.
9. Batzofin, .T.H., Fieding, W.L. and Friedman, A.E. Effect of vaginal bleeding in early pregnancy outcome. Obstet. Gynecol., 1984;63 :515-8.
10. Sipila. P., Oja, H. and Wendt, L. Perinatal outcome ofpregnancics complicated by vaginal bleeding. Br. J.Obstet. Gynecol., 1992;99:959-63.
11. Chamberlain, G.V.P The epidemiology ofperinatal loss. In Studd, J. eds. Progress in Obstetrics and Gynaccology, Vol. 1, Edinburgh, Churchill Livingstone, 1981, p. 10.
12. Villar, J., Altobelli, L., Kestler, E. et al. A health priority for developing countries: The prevention of chronic fetal malnutrition. Bull. WHO., 1986;64:847-851.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: