
Asma Nasim ( Department of Infectious Diseases, Sindh Institute of Urology and Transplantation, Karachi. )
Shehla Baqi ( Department of Infectious Diseases, Sindh Institute of Urology and Transplantation, Karachi. )
Syed Mohammed Zeeshan ( Department of Microbiology, Sindh Institute of Urology and Transplantation, Karachi. )
Tahir Aziz ( Department of Nephrology, Sindh Institute of Urology and Transplantation, Karachi. )
December 2011, Volume 61, Issue 12
Case Reports
Abstract
Chronic necrotizing pulmonary aspergillosis is a chronic semi invasive pulmonary disease. It is an uncommon disease and has never been reported in transplant recipients. We report a case of chronic necrotizing pulmonary aspergillosis in a renal transplant recipient.
Keywords: Fungal infections, Renal transplantation, Pulmonary aspergillosis.
Introduction
Aspergillus is a mold with over 100 species. Aspergillus fumigatus, A.flavus A. terreus and A. niger are known to cause invasive disease in humans.1 Four distinct clinical syndromes of the lung are described; allergic bronchopulmonary aspergillosis, aspergilloma, chronic necrotizing aspergillosis, and invasive pulmonary aspergillosis.
The incidence of invasive fungal infections in kidney transplant recipients is 1-14% with 74% occurring within the 1st year of transplantation.2 In transplant and immunocompromised patients, pulmonary aspergillosis may rapidly progress to invasive disease with a mortality of around 63%.3
Chronic necrotizing pulmonary aspergillosis (CNPA) is an uncommon invasive pulmonary infection with a slow and indolent course.4 We present a case of chronic necrotizing aspergillosis in a patient on immunosuppressive therapy due to renal transplantation. To the best of our knowledge, CNPA has not been reported as such in transplant recipients.
Case Report
A 35 year old male received live related renal transplant in August 2009 and was placed on prednisolone, azathioprine and cyclosporine. Seven months later he presented with productive cough, haemoptysis and low grade fever since two weeks. Chest X-ray showed a mass in the left apical region of the lung. Sputum and bronchoalveolar lavage were negative for acid fast bacilli, but based on history and radiological findings he was started on antituberculous therapy (ATT) empirically.
His symptoms persisted with fever, worsening cough and chest pain despite 2 months of ATT, although he remained stable and had no respiratory distress. CT chest showed a soft tissue mass 5.6 4cm with central necrosis and air lucency in the apical region (Figure-1).
CT guided biopsy showed broad aseptate hyphae with right angled branching and background necrosis. Mucormycosis was diagnosed on the basis of the histopathology report and he was started on Inj. amphotericin B deoxycholate 1.5mg/kg/day. Surgical resection of the mass with left upper lobectomy was performed. Histopathology showed septate hyphae with acute angle branching and back ground necrosis (Figure-2).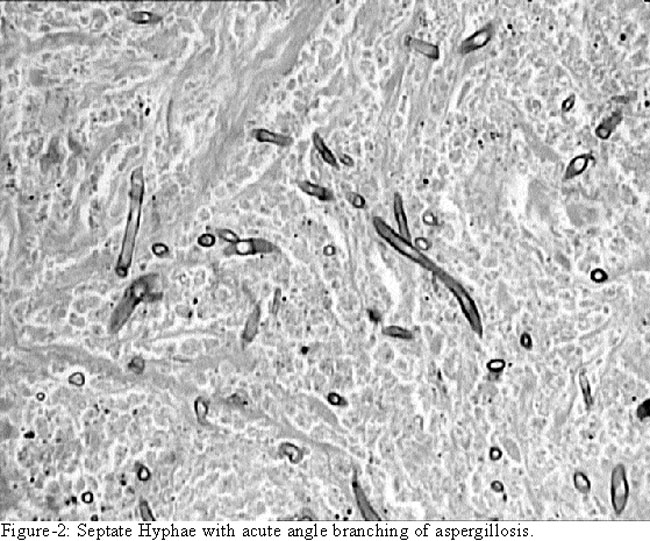
Culture of the specimen grew Aspergillus fumigatus. There was no evidence of mucormycosis.
Post operative period was complicated by lower lobe collapse and gram negative bacteraemia, and patient recovered slowly. Amphotericin B was continued for 6 weeks and then he was placed on oral itraconazole 200mg twice daily.
Discussion
The clinical spectrum of pulmonary aspergillus can range from colonization of a previous lung cavity to parenchymal and vascular invasion.4 In 1981, Gefter et al described a semi-invasive type of pulmonary aspergillosis, later known as chronic necrotizing pulmonary aspergillosis.5
CNPA is a chronic, indolent and locally invasive disease with slowly progressive cavitation.4 There is no vascular invasion or dissemination to other organs. It is seen commonly in patients with altered local or systemic immune defenses or with preexisting lung disease like COPD, bronchiectasis, or pneumoconiosis.6
Average age at presentation is 40-50 years. Most common symptoms are chronic productive cough, weight loss, fever and chest pain. Haemoptysis, dyspnoea and finger clubbing can also occur.4
Radiologically CNPA commonly involves the upper lobes of the lungs with progressive cavitation and pleural thickening occurring over weeks or months. Initially there is pulmonary opacification which progresses to necrosis with a central cavity (air crescent sign). It can be differentiated froms an aspergilloma by the fact that an aspergilloma resides in a cavity while CNPA form its own cavity slowly over weeks or months. Transbronchial and percutaneous biopsy have low diagnostic yields for locally invasive aspergillosis. Sputum culture has a sensitivity of only 50-60% in CNPA.6
The diagnostic criteria for CNPA are a) chronic symptoms of fever, cough and weight loss b) CXR and CT findings of infiltration and cavitations in the upper lobe, c) positive antibody test and /or d) isolation of Aspergillus spp. from the lung specimens e) failure to detect other bacterial, fungal or mycobacterial pathogen.7 Our patient met the above diagnostic criteria.
An average delay of 1-6 months is reported for the diagnosis of CNPA leading to increased morbidity and mortality.4 Hence Saraceno et al suggested early diagnosis by prompt recognition of symptoms and radiological changes in high risk patients.4
Graft dysfunction, intensive immunosuppression, renal failure and need for dialysis are the main risk factors for the development of invasive aspergillosis in solid organ transplant recipients. Often such patients do not manifest typical signs and symptoms.8
The principles of therapy for CNPA are similar to those for invasive pulmonary aspergillosis.9 Itraconazole 400mg daily , amphotericin B deoxycholate up to a total dose of 2 gms if itraconazole treatment fails and combination therapy in refractory cases has been recommended. In the setting of clinical deterioration intra-cavitatory instillation of amphotericin can also be considered.4 In renal transplant patients Voriconazole is found to be very effective in invasive aspergillosis.3 However interaction of Voriconazole with calcineurin inhibitors leads to their increased plasma levels requiring careful monitoring to avoid toxicity. Duration of therapy has not been well defined. A minimum of 6-12 weeks has been recommended. In patients on immunosuppressive therapy, decrease in immunosuppression or continuation of antifungals as long as the patient is on immunosuppressives is suggested.9 Surgical resection may be beneficial in selected patients. Sugino et al reported that in CNPA, aspergillus can invade the vessels in the cavity wall which can lead to severe haemoptysis and even death and surgical resection can improve the patient outcome.7
The reported mortality is variable (10% to 38%) and further studies are needed.4 Recently Neophytos et al report a mortality of 29.6% over 12 weeks in solid organ transplant recipients.10
Conclusion
In conclusion CNPA is a rare disease which needs early recognition and prolonged therapy to prevent complications and to improve patient outcome.
References
1.Patterson TF, Kirkpatrick WR, White M, Hiemenz JW, Wingard JR, Dupont B, et al. Invasive aspergillosis. Disease spectrum, treatment practices, and outcomes. 13 Aspergillus Study Group. Medicine (Baltimore) 2000; 79: 250-60.
2.Einollahi B, Lessan-Pzeshki M, Pourfarziani V, Nemati E, Nafar M, Pour-Reza-Gholi F, et al. Invasive fungal infections following renal transplantation: A review of 2410 recipients. Ann Transplant 2008; 13: 55-8.
3.Ju MK, Joo DJ, Kim SJ, Chang HK, Kim MS, Kim SI, et al. Invasive pulmonary aspergillosis after solid organ transplantation: diagnosis and treatment based on 28 years of transplantation experience. Transplant Proc 2009; 41: 375-8.
4.Saraceno JL, Phelps DT, Ferro TJ, Futerfas R, Schwartz DB. Chronic necrotizing pulmonary aspergillosis: approach to management. Chest 1997; 112: 541-8.
5.Gefter WB, Weingard TR, Epstein DM, Ochs RH, Miller WT. "Semi-invasive" pulmonary aspergillosis: a new look at the spectrum of Aspergillus infections of the lung. Radiology 1981; 140: 313-21.
6.Prasad R, Garg SR. Progressive increase in cavitation with the evolution of fungal ball: a clue to the diagnosis of chronic necrotizing pulmonary aspergillosis. Lung India 2009; 26: 95-7.
7.Sugino K, Hasegawa C, Sano G, Shibuya K, Homma S. Pathophysiological study of chonic necrotizing pulmonary aspergillosis. Jpn J Infect Dis 2008; 61: 450-3.
8.Sheppard D, Grist LM. Report from the Fourth Advances Against Aspergillosis Conference. Future Microbiol 2010; 5: 1001-4.
9.Walsh TJ, Anaissie EJ, Denning DW, Herbrecht R, Kontoyiannis DP, Maw KW, et al. Treatment of Aspergillosis: Clinical Practice Guidelines of the Infectious Diseases Society of America. Clin Infect Dis 2008; 46: 327-60.
10.Neofytos D, Fishman JA, Horn D, Anaissie E, Chang CH, Olyaei A, et al. Epidemiology and outcome of invasive fungal infections in solid organ transplant recipients. Transpl Infect Dis 2010; 12: 220-9.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: