
Aslam Khan ( Department of Medicine, Combined Military Hospital, Quetta. )
Azhar Ali Chaudhry ( Department of Medicine, Combined Military Hospital, Quetta. )
Uzair Khan ( 4th Year MBBS student, AM College, Rawalpindi. )
January 2012, Volume 62, Issue 1
Case Reports
Abstract
The case of a 23-year-old male presenting with a rash on the chest and lower limbs is presented. Work up revealed bicytopenia and plasmodium falciparum on bone marrow biopsy. Treatment with antimalarial drugs resulted in resolution of haematological abnormalities and rash.
Keywords: Falciparum, Thrombocytopenia, Petechiae.
Introduction
Malaria is the second largest killer of humanity after tuberculosis in tropical countries. Despite its common occurrence, it can sometimes befool the most astute of physicians. Diagnosis of malaria often requires high index of suspicion as patients may have highly atypical presentation. This is especially true of plasmodium falciparum infections, which if unrecognized may have a fulminant course with disastrous consequences. Falciparum malaria can very rarely present with cutaneous manifestations like purpura fulminans, acute urticaria, angioedema, and petechiae.1
We describe an unusual case of falciparum malaria presenting with purpuric rash in an otherwise asymptomatic person.
Case Report
A 23-year-old serving soldier was admitted with a non pruritic skin rash on the chest and legs of one week duration (Figure).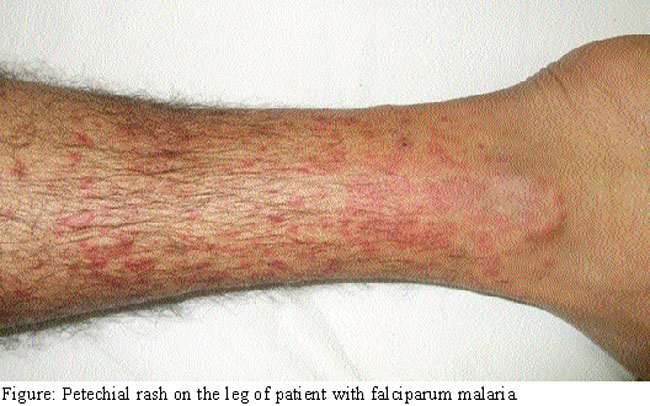
There was no history of fever, gum bleed, malena, epistaxis, cough, arthralgias, or insect bite. On examination the patient was afebrile. There was no pallor, icterus, fundal haemorrhages or lymphadenopathy. Systemic examination did not reveal any abnormality. Dermatological examination showed diffuse non palpable petechial rash on the chest anteriorly and on both the legs involving the shins and ankles. Laboratory investigation revealed haemoglobin of 15.6 gm/dl, total leucocyte count of 2600/ mm3, (differential leucocyte count polymorphs 67%, lymphocytes 23%, monocytes 6%, eosinophils 4%) platelets 02 x 109/ul . Repeated peripheral blood smears (thick and thin) were negative for malarial parasites. All other investigations including liver and renal function tests, Prothrombin time, Fibrinogen levels, fibrinogen degradation products, blood cultures, radiograph of chest and ultrasound of the abdomen were normal. Rheumatoid factor, antinuclear factor and serologies for hepatitis B, C and Dengue virus were negative.
Bone marrow biopsy revealed trophozoites and ring forms of falciparum. Alongwith platelet transfusions, oral artemether plus lumefantrine were started. Patient\\\'s leucocyte count returned to normal and rash settled in a week\\\'s time, while platelets returned to normal after about two weeks of treatment. Follow up platelet counts after 4 weeks of discharge from hospital were within normal range.
Discussion
Malaria has infected humans for over 50,000 years, and is widespread in tropical and subtropical regions. It is transmitted by the bite of infected Anopheles mosquitoes. It is the most important of the parasitic diseases of humans, with transmission in 107 countries containing 3 billion people and causing 1-3 million deaths each year.2 Four species of the genus Plasmodium cause nearly all malarial infections in humans. These are P. falciparum, P. Vivax, P. ovale, and P. malariae.
The common symptoms to all forms of malaria are paroxysmal fever spikes, chills, rigors, headache, fatigue, nausea, and vomiting. While major manifestations of severe falciparum malaria are cerebral malaria, acidosis, bone marrow suppression, renal failure, adult respiratory distress syndrome, hypoglycaemia, shock, disseminated intravascular coagulation, convulsions and haemoglobinuria.3,4 Presentations like acute abdomen, clinical picture of lower respiratory tract infection, and acute hepatitis with fulminant hepatic failure are rare manifestations of falciparum infection.5,6
Dermatological manifestations like petechiae which are small (1-2mm) red or purple spots on the body, caused by a minor haemorrhage(a sign of thrombocytopenia, platelet function disorder, or in clotting factor deficiencies) seen in meningococcal septicaemia, typhus, enteric fever, viral exanthems, and drug reactions are very rare with malaria and are mainly seen with falciparum species.
There are only few case reports, in the literature which cite instances of falciparum malaria presenting with acute skin rash.7
The patient under discussion had only petechial rash on chest and legs at the time of presentation. His blood complete picture revealed leucopenia and severe thrombocytopenia which raised the possibility of malaria. Although, repeated peripheral smears for malarial parasites were negative, bone marrow biopsy did help uncover the culprit falciparum causing acute bone marrow suppression and skin rash. As bicytopenia and rash settled with antimalarial treatment, and other common causes of petechial rash and bicytopenia were ruled out with appropriate investigations, hence, we can safely say that the rash and bicytopenia in our patient was due to falciparum malaria.
Conclusion
Malaria remains a diagnostic and treatment challenge for clinicians as increasing numbers of patients present with atypical manifestations. This case highlights the importance of considering the possibility of malaria in patients presenting with petechial rash especially in endemic areas like Baluchistan.
References
1.Keri JE, Thomas K, Berman B, Falabella A. Purpura fulminans in a patient with malaria. Eur J Dermatol 2000; 10: 617-9.
2.Snow RW, Guerra CA, Noor AM, Myint HY, Hay SI. The global distribution of clinical episodes of Plasmodium falciparum malaria. Nature 2005; 434: 214-7.
3.Ladhani S, Khatri P, El-Bashir H, Shingadia D. Imported malaria is a major cause of thrombocytopenia in children presenting to the emergency department in east London. Br J Haematol 2005; 129:707-9.
4.Mahmood K, Jairamani KL, Abbasi B, Mahar S, Samo AH, Talib A, et al. Falciparum malaria: various presentations. Pak J Med Sci 2006; 22: 234-377.
5.Bhalli MA, Samiullah. Falciparum malaria - A review of 120 cases. J Coll Phys Surg Pak 2001; 11: 300-3.
6.Ahsan T, Rab SM. Falciparum malaria or fulminant hepatic failure? J Pak Med Assoc 1993; 43: 206-8.
7.Mitra A. Malaria presenting with urticaria as the initial feature. Indian Pediatr 1989; 26: 728.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: