
Akbar Pirzadeh ( Department of Surgery School of Medicine, Tehran University of Medical Science, Tehran, Iran. )
Mohammad Khorsandi ( Department of Nursing, School of Nursing, Tehran University of Medical Science, Tehran, Iran. )
Mohammad-Ali Mohammadi ( Department of Otolaryngology, School of Medicine, Tehran University of Medical Science, Tehran, Iran. )
Ahmad Pirzadeh ( Department of Surgery School of Medicine, Tehran University of Medical Science, Tehran, Iran. )
July 2011, Volume 61, Issue 7
Original Article
Abstract
Objective: Cochlear implantation (CI) is an effective treatment for profound deaf patients. To study the cochlear implant complications in patients at Amir Aalam Hospital.
Methods: The study population involved 177 profoundly deaf patients, implanted within the same cochlear implant center.
Results: Twenty-four (13.6%) patients experienced complications. Early complications accrued in 9 (37.7%) patients within the first 24 hours. Eight (4.5%) patients had major complications including facial nerve paralysis, suture rupture and prosthesis rejection. Prosthesis rejection 6 (30%) was the most frequent major complication. Minor complications were found in 16 (9%) cases which were managed medically. Older age with CI was correlated with higher major complications.
Conclusion: In contrast to minor complications, the frequency of major complications in this cohort was higher than that published by other groups.
Keywords: Cochlear implantation, Complications, Iran (JPMA 61:622; 2011).
Introduction
Cochlear implantation (CI) is the reference treatment of profound sensorineural hearing loss. Implantation of cochlear entails a surgical procedure with the attendant potential for complications. In response to good results from implantation, the candidacy criteria have gradually been relaxed, with the implant devices now being used for children as young as 12 months.1-3
Not enough data is available about the possible complications after CI, especially in the developing country context.4 Complications of CI are not only important from the standpoint of patient care, but they also add significantly to length of hospital stay and increase health care costs.5
In this study, we describe the complications in a cohort of patients consecutively treated in a single center with CI. The frequency of the implantations in the cohort was compared with previous studies.
Methods
All consecutive patients referred to the Amir Aalam Hospital, Iran for the CI from January 1997 to January 2007 were included in this study. Data in the CI database were collected by an ear specialist and a research coordinator at the hospital. We collected data on patients\\\' characteristics, indication for CI, and implant related details. We also collected clinical and implant related events occurring in the follow-up.
The indication for CI was based on international recommendations.6 All patients were fitted with the MED-EL C40+ cochlear implant and used the behind-the-ear TEMP+ speech processor. The devices used were the nucleus (Cochlear Ltd.) or the Clarion (Advanced Bionic Corp.). Selections of these patients followed the criterion that they had complete three-year data on the questionnaires. At the cochlear clinic visits and follow-up contacts after device implantation, patients were routinely evaluated for any device-related complications that occurred within 3 years of the implantation surgery. These complications were categorized as major or minor based on the consensus of the ear specialist. Clinical complications were considered to be major if hospitalization and/for additional surgery were required. Minor complications were defined as complications requiring a minor procedure at office sitting or resolved spontaneously or with medical therapy.
Data were expressed as mean ± standard deviation or as median as appropriate. Correlation analyses were performed with the Pearson correlation coefficient method. A p value <0.05 was considered to indicate a statistically significant difference. All analyses were carried out using SPSS for windows version 11.0 (SPSS Inc.).
Results
The final study cohort consisted of 177 patients, and their characteristics are shown in Table 1.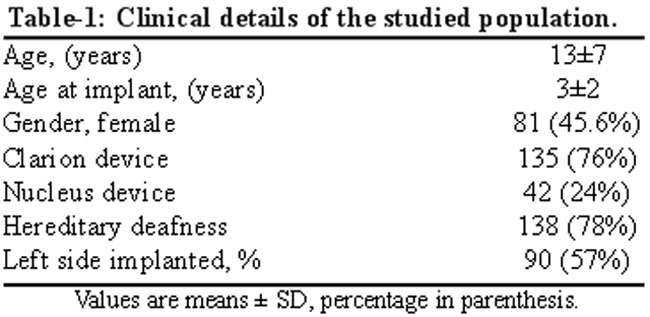
The patients age at implantation ranges from 6 months to 60 years with a mean age at implantation of 3 ± 2 years. There were 96 males and 81 females in the sample. Follow-up data for complications were available for all patients. The majority of patients had hereditary deafness, and nearly 89% were below the age of 10. A total of 24 (13.6%) patients experienced related complications. There was no significant difference in overall complication rate by gender. Major and minor complications occurred in 8 (4.5%) and 16 (9%) patients. A large proportion of complications occurred in the first 24 hours after surgery, at rate of 37.7% for complications. The most frequent major complications were prosthesis rejection (5%) (Table 2).
The age of these patients at CI were 1, 2 and 3 years. All of them had cholesteatoma and a granular reaction to the ear undergoing implantation 9 months after surgery. Four of these patients underwent reimplantation with success. Two patients underwent cochleostomy without reimplantation. The record causes of prosthesis rejection included wearing a hat which can cause pressure on flap, previous mastoid surgery or previous scar. Wearing of a hat (r=0.35, P=0.001) and age at CI (r=0.31, P=0.02) were positively correlated to prosthesis rejection. The suture rupture occurred in a 3-year-old girl. She underwent general anaesthesia and prosthesis was repositioned and fixed into the cochlear. Apart from local inflammation, there were no severe infectious complications (such as meningitis).
Minor complications occurred in 16 patients. Incisional infections and pocket haematomas that did not require operative procedure were the most common minor complications. Partial facial paralysis occurred in a 1-year age child, which resolved by nerve decompression in two months. Cutaneous haematoma developed in 5 patients. Successful outcome was achieved with local dressing and antibiotic therapy.
The overall outcome of CI was satisfactory. Most patients could communicate without visual help within 2-3 months and they could hear and talk on the telephone with a known speech in about a year.
Discussion
CI has emerged as an effective therapeutic option for patients with sensorineural hearing loss. The results of this study revealed a wide range of complications in patients implanted at Amir Aalam Hospital. The overall incidence of CI complications was 13.6% in the studied population, 4.4% for major and 8.8% for minor complications. The present results are different from those of Bhatia et al.7 and Hashemi et al.8 who reported an incidence of complications of 18% (2.3% major and 16% minor) and 12.7% (2.7 major and 10% minor) respectively.9 The present high incidence of complication also contracts with reports on children in which complications are observed in up to 3% patients. The inappropriate recording for these patients could explain the lower incidence of minor CI complications as compared with other reports. Previous studies have reported that flap problems, cholesteatoma and tampon perfusion were the most common major events.7
Prosthesis rejection is quite an important issue in the studied population, because it could not be resolved by revision surgery. Although it was not the aim of our study, we observed that wearing of hat and age at CI were correlated to prosthesis rejection. Our results underline the necessity of reevaluating current eligibility criteria for implant candidacy.10
The flap failures have been identified as one of the most common CI complication, which can be resolved by using post-auricular- instead of C-shaped incision.11 Consistently, all the study patients underwent post-auricular-shaped incision.
The frequency of major complications is high enough to require adequate post-surgery monitoring. It is evident that not all types of complications were reported by different investigators. These observations suggest that comparisons among articles should be done with caution and underlines the lack of extensive experience with CI.
References
1.Hall WH. NIH statement on cochlear implants. CMAJ 1996; 155: 20.
2.Gifford RH, Dorman MF, Shallop JK, Sydlowski SA. Evidence for the expansion of adult cochlear implant candidacy. Ear Hear 2010; 31: 186-94.
3.Valencia DM, Rimell FL, Friedman BJ, Oblander MR, Helmbrecht J. Cochlear implantation in infants less than 12 months of age. Int J Pediatr Otorhinolaryngol 2008; 72: 767-73.
4.Zeng FG. Trends in Cochlear Implants. Trends Amplif 2004; 8: 1-34.
5.Cheng AK, Rubin HR, Powe NR, Mellon NK, Francis HW, Niparko JK. Cost-utility analysis of the cochlear implant in children. JAMA 2000; 284: 850-6.
6.Waltzman SB. Cochlear implants: current status. Expert Rev Med Devices 2006; 3: 647-55.
7.Bhatia K, Gibbin KP, Nikolopoulos TP, O\\\'Donoghue GM. Surgical complications and their management in a series of 300 consecutive pediatric cochlear implantations. Otol Neurotol 2004; 25: 730-9.
8.Hashemi B, Bayat A, Kazemei T. Surgical complications of cochlear implantation. Iran J Med Sci 2010; 35: 53-6.
9.Lin YS, Lee FP, Peng SC. Complications in children with long-term cochlear implants. ORL J Otorhinolaryngol Relat Spec 2006; 68: 237-42.
10.Nikolopoulos TP, O\\\'Donoghue GM, Archbold S. Age at implantation: its importance in pediatric cochlear implantation. Laryngoscope 1999; 109: 595-9.
11.Schweitzer VG, Burtka MJ. Cochlear implant flap necrosis: adjunct hyperbaric oxygen therapy for prevention of explantation. Am J Otol 1991; 12: 71-5.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: