
Foad Ali Moosa ( Surgical Unit-I, Dow University of Health Sciences, Civil Hospital, Karachi. )
Fazal Wahab Khan ( Surgical Intern, Dow University of Health Sciences, Civil Hospital, Karachi. )
Masood Hussain Rao ( Research Officer, PMRC, Dow University of Health Sciences, Civil Hospital, Karachi. )
August 2010, Volume 60, Issue 8
Original Article
Abstract
Objectives: To determine the effectiveness of the circumcision by Plastibell technique with comparison of complications among neonate and infant age groups.
Methods: A retrospective, descriptive study was conducted in all the plastibell circumcisions performed by the first author, during the period October 2006 to December 2008 at a private hospital Karachi. The record of all the cases fulfilling the inclusion criteria were obtained and analyzed for determining the outcome and complications if any in neonates and infants and to compare it with in these two groups.
Results: Overall 245 cases of neonates and infants were selected. Mean age of neonates and infants was 14 ± 2 days and 3 ± 0.5 months respectively. The plastibell circumcision was done in all the cases i.e. 90 neonates and 155 infants. Out of these, the successful rate of plastibell circumcision without any complication was recorded as 196 cases (80.00%) whereas, 49 cases (20.00%) developed complications. In neonates it was recorded as 04.44 % cases, whereas this ratio was 29.03 % in infants.
Most common complications were delayed separation of the ring in 17 cases (6.93%), bleeding in 12 cases (4.89%), localized superficial infection in 12 cases (4.89%), and proximal migration of ring in 07 cases (2.85%).
Conclusion: The ratio of complications of circumcision by plastibell is significantly higher in infants as compared to neonates. However it is an easy, quick and safe technique. Outcome of this procedure is encouraging while infants are more prone to develop post operative complications than neonates (JPMA 60:664; 2010).
Introduction
Circumcision is perhaps the commonest operation in surgery. Throughout the world, millions of male neonates and infants undergo circumcision for religious, cultural, social and medical reasons.1,2 In Pakistan, it is generally observed that the majority of males undergo circumcision from newborn to adulthood, nevertheless, it is more commonly practiced in the first year of life. It is a simple operation in both infants and young children and healing is usually complete within two weeks.
Various techniques are available for circumcision, namely Plastibell, Gomco clamp, Mogen clamp, bone cutter method and dorsal slit (open cut) method.3 Out of these, Plastibell method has become quite popular and appears to be the more preferable procedure particularly in the age group ranging from neonates to one year of age. It is because of being a quick, easy, least traumatic technique with minimal blood loss and having least number of complications. It also provides very good cosmetic results.3,4
However, complications of Plastibell circumcision include bleeding, bell impaction, localized infection, dysuria, inadequate skin removal, excessive loss of skin, incomplete separation of Plastibell device, proximal migration of the ring under the prepuce with prolapse of glans through the ring.1
Plastibell circumcision like any other surgical procedure requires an aseptic technique with sterilized instruments, drapes, antiseptic solution, and local anaesthesia in the form of dorsal penile block and/or ring block.4 The use of local anaesthesia for the procedure is recommended for neonates and for older children.5 Coagulation profile is a mandatory prerequisite for circumcision but is not routinely practiced except where family history of coagulopathy is present.6
The operating time of the procedure exclusive of local anaesthesia is 5 to 10 minutes. The pain management for this procedure proves to be helpful but not perfect. The dorsal penile block seems to be inadequate on its own, but in combination with penile ring block gives much better results for pain control, though penile ring block may result in bruising and haematoma formation.3
The plastibell ring device is available in sizes ranging from 1.1cm to 1.7cm and is correlated to the size of the glans of penis. An appropriate bell size which snugly fits in 2/3 of the glans should be used along with the thread that is tight enough to cause ischaemia of the foreskin. If the thread is not securely tightened or if the skin is too thick as in older children, it will result in incomplete/delayed separation of the ring. Smaller bell size will results in tissue necrosis and larger bell can migrate proximally and get impacted. If the complications are established in a particular technique, it is easier for the surgeons to decide to use according to the appropriate age group. Therefore, this study was conducted to determine the effectiveness of the circumcision using Plastibell technique with comparison of complications among neonates and infants.
Methods
A retrospective descriptive study was conducted in all Plastibell circumcisions at a private hospital of Karachi during October 2006 to December 2008. All records of Plastibell circumcisions were retrieved. The patients were divided into two groups: neonates (0 to 4 weeks) and infants (5 to 52 weeks). Only the data of healthy neonates and infants who had undergone Plastibell circumcision were included in the study. In all the cases, preoperative examination was done. To avoid vomiting and possible aspiration, parents were advised to stop feeding the neonates or infants for 1 to 2 hours prior to surgery. Verbal consent was taken from either of the parents describing all the benefits and adverse effects that might occur after the procedure. Records of all patients who had congenital abnormalities like hypospadias, deep jaundice, de-ranged coagulation profile, extensive skin nappy rash, and any other medical illnesses were excluded. The data was analyzed through SPSS version 15.0. Frequencies and percentages were calculated for variables. Chi-Square as test of significance was applied to compare the two groups and p < 0.05 was considered as statistically significant.
Procedure of Plastibell Circumcision:
In this procedure a plastic ring fits around the glans and a strong thread is tightened around it. This thread will cut the blood supply from the foreskin which will eventually die and fall off with the ring within 1 to 2 weeks.
Aseptic measures were ensured, local anesthesia in the form of Dorsal penile block and ring block using 1cc of lignocaine (1%) in a disposable insulin syringe was given in all cases. The procedure was assisted by one trained nurse. The foreskin was separated from the glans by using a blunt curved artery forceps and gauze, following which a dorsal slit was made on the foreskin until the corona glandis was visible. An appropriate size of Plastibell which snugly fits in 2/3 of the glans was then placed on the glans and the foreskin brought over it. This was then secured with a cotton thread supplied with the Plastibell. The foreskin was then trimmed and the handle of the ring snapped (Figure-1).
Following the procedure, oral analgesic drops and local antibiotic ointment was given to the parents. All neonates and infants were called for 1st follow-up after two days and were told to contact earlier, in case of any complication arises. In those patients in which the ring was not separated within 1-2 weeks were called for 2nd follow-up and the ring was removed by cutting the thread and excision of the necrotic foreskin with or without local anaesthesia. A ring cutter was used to remove the ring (if required). Complete record of these patients was maintained during the follow-up.
Results
During the study period, 245 cases of Plastibell circumcision fulfilling the inclusion criteria were included and analyzed. Out of the total cases, 90 (36.73%) were neonates, whereas the remaining 155 (63.26%) were infants. Mean age of the neonates was 14 ± 2 days whereas that of infants was 3.0 ± 0.5 months.
Out of the total 245 cases, the successful rate of Plastibell circumcision without any complication was recorded in 196 (80%) cases. The remaining 49 (20%) cases developed minor complications. In neonates, out of 90 cases only 04 (4.44%) developed complications. The most common was delayed separation of the ring, recorded in 02 cases (2.22%). In infants, out of 155 cases, 45 (29.03%) developed complications; the most common was delayed separation of the ring in 15 (9.67%) cases.
According to the comparison of different complications in neonate and infant age groups, delayed separation of the ring was the highest and was recorded in 17 cases. This complication developed in only 02 of neonates. Other complications included bleeding in 12 cases (1 neonate and 11 infants) and localized superficial infection in 12 cases (1 neonate and 11 infants) (Figure-2).
Complications of delayed separation of the ring, bleeding, localized superficial infection and proximal migration of ring was found to be statistically significant when neonates and infants were compared (p < 0.05) (Table).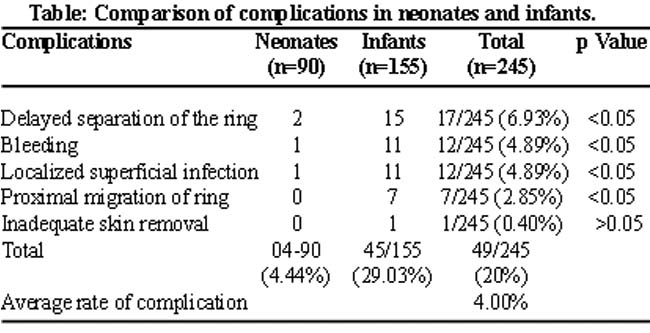

Discussion
The technique of Plastibell circumcision has established itself as an acceptable form of circumcision particularly in neonates to one year old infants. Complications with this technique are reported to be 2% to 3%.2,7,8 Most common of which are bleeding and local infection.2,3,7 Other minor complications include bell impaction, dysuria, incomplete separation of Plastibell device, proximal migration of the ring, inadequate skin removal and excessive loss of skin.9 However, case reports of significant complications have also been documented that includes necrotizing fasciitis, urinary retention and ischaemic necrosis of the glans.7
In our study, the complications observed were delayed separation of ring, bleeding, localized superficial infection, proximal migration of ring, and inadequate skin removal. The average rate of occurrence of any of the above complications in both neonates and infants was 4% which is nearer to studies done internationally.2,7,8
Studies have documented that the residual plastic ring usually falls off within 10 days of the procedure.10 while the ring separates faster in neonates due to thin prepuce and easier sloughing.11 In the present study, ring separation in lesser time was faster in neonates than infants was also observed due to thin prepuce and easier sloughing. Among those (6.93%) whose bell did not separate by spontaneously within 10 days, the ring was removed by cutting the tied knot. However, close attention is required during Plastibell technique, to ensure that the ligature is tightened appropriately around the ring to prevent bleeding and possibility of delayed separation of the ring.
In this study, Plastibell ring migrated proximally and was stuck in 07 cases (2.85%) and was removed manually. It has been documented that a ring too large may result in much of the foreskin being removed and penile denudation. It may also slip or migrate proximally and get proximally stuck on the glans with prolapse of glans through the ring.1,7,12 Also smaller size ring can get impacted on the glans and can cause tissue strangulation and necrosis. Surgeons should remain conscious in selecting the correct bell size which snugly fits in 2/3 of the glans.
The most widely studied pharmacological intervention for pain management during circumcision is dorsal penile block by injecting 1% lignocaine and randomized controlled trials have demonstrated its efficacy.13 If untreated, the pain of circumcision causes both short and long term changes in infant behaviours. Infants pre-medicated with lignocaine have significantly smaller changes in physiological and pain related behaviours compared with infants who are not given analgesics.13 A meta-analysis of local anaesthetic injection related adverse effects including bruising and haematoma which yielded a risk of 6.7% with no systemic toxicity.13 Regarding effective local anaesthesia and pain control by ring block, another study reports that a ring block using 1ml of 0.5% lignocaine delivered subcutaneously and circumferentially at the base of the penis significantly attenuates circumcision induced pain, increase in heart rate, and crying and decrease in O2 saturation.14 Less effective modalities includes topical anaesthesia with lignocaine-prilocaine cream, EMLA (Eutectic mixture of local anaesthetics)13 In the present study, 90 cases were neonates and by using combined dorsal and ring block using 1% lignocaine was found to be effective as a few patients felt discomfort and complications after surgery.
Circumcision performed in the neonatal period had better results with fewer complications in comparison to older infants. This is because newborn babies have a thin and soft skin that comes off easily therefore causing minimum complications and has been observed in both local and international studies6,15 and the present study confirms this claim.
In our society, conventional method of circumcision has long been adopted with the use of bone cutter for homeostasis. It is important to emphasize that trauma to glans results in a well-known and dangerous complication of partial amputation of the glans is more common with bone cutter circumcision16 and should be discouraged.
Conclusion
Plastibell circumcision in is an easy, quick and safe technique while the ratio of complications of circumcision by Plastibell is significantly higher in infants as compared to neonates. It is recommended that this technique should preferably be performed in the neonatal period as infants are more prone to develop post operative complication.
References
1.Shah T, Raistrick J, Tailor I, Young M, Menebhi D, Stevens R. A circumcision service for religious reasons. BJU International 1999; 83: 807-9.
2.Palit V, Menebhi DK, Taylor I, Young M, Elmasry Y, Shah T. A unique service in UK delivering Plastibell circumcision: review of 9-year results. Paediatr Surg Int 2007; 23: 45-8.
3.Rafiq K. Plastibell-A quick technique to decrease the distress of neonatal circumcision. Ann King Edward Med Coll 2000; 6: 412-3.
4.Khan NZ. Circumcision- A universal procedure with no uniform technique and practiced badly. Pak J Med Sci 2004; 20: 173-4.
5.American Academy of Pediatrics. Circumcision policy statement. Task Force on Circumcision. Pediatrics 1999; 103: 686-93.
6.Jan IA. Circumcision in babies and children with Plastibell technique: an easy procedure with minimal complications- experience of 316 cases. Pak J Med Sci 2004; 20: 175-80.
7.Lazarus J, Alexander A, Rode H. Circumcision complications associated with the Plastibell device. S Afr Med J 2007; 97: 192-3.
8.Manji KP. Circumcision of the young infant in a developing country using Plastibell. Ann Trop Paediatr 2000; 20: 101-4.
9.Mihssin N, Moorthy K, Houghton PW. Retention of urine: an unusual complication of the Plastibell device. BJU Int 1999; 84: 745.
10.Duncan ND, Dundas SE, Brown B, Pinnock-Ramsaran C, Badal G. Newborn circumcision using the Plastibell device: an audit of practice. West Indian Med J 2004; 53: 23-6.
11.Mousavi SA, Salehifar E. Circumcision complications associated with the Plastibell device and conventional dissection surgery: A trial of 586 infants of ages up to 12 months. Adv Urol 2008; 2008: 606123.
12.Williams N, Kapila L. Complications of circumcision. Br J Surg 1993; 80: 1231-36.
13.Taddio A. Pain management for neonatal circumcision. Paediatric Drugs 2001; 3: 101-11.
14.Hardwick-Smith S, Mastrobattista JM, Wallace PA, Ritchey ML. Ring block for neonatal circumcision. Obstet Gynecol 1998; 91: 930-34.
15.Christakis DA, Harvey E, Zerr DM, Feudtner C, Wright JA, Connell FA. A trade-off analysis of routine newborn circumcision. Paediatrics 2000; 105: 246-9.
16.Rehman J, Ghani U, Shehzad K, Sheikh IA. Circumcision - A comparative study. Pak Armed Forces Med J 2007; 57: 286-8.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: