
Arshad Mehmood Malik ( Department of Surgery, Liaquat University of Medical & Health Sciences, Jamshoro, Sindh, Pakistan. )
Shiraz Sheikh ( Department of Surgery, Liaquat University of Medical & Health Sciences, Jamshoro, Sindh, Pakistan. )
Asad Khan ( Department of Surgery, Liaquat University of Medical & Health Sciences, Jamshoro, Sindh, Pakistan. )
Ubedullah Sheikh ( Department of Surgery, Liaquat University of Medical & Health Sciences, Jamshoro, Sindh, Pakistan. )
August 2010, Volume 60, Issue 8
Original Article
Abstract
Objectives: To study the spectrum of presentation and outcome of different treatment modalities in Fournier\'s gangrene.
Methods: It\'s a prospective analysis of 73 diagnosed patients of Fournier\'s gangrene admitted and treated in surgical department of a public sector university from June 2000 to June 2008. All patients were admitted through casualty with varying proportions of necrotizing infection of the perineal and genital fascia, with gangrene of the overlying skin. After resuscitation and preliminary investigations, including culture of the necrotic tissue, the patients were treated either conservatively by broad spectrum antibiotics, cardiopulmonary support, nutritional and fluid support or surgically by repeated aggressive wound debridement under anaesthesia. The behaviour of the disease, different modalities of treatment offered, response and outcome of the management were all collected on a proforma for statistical analysis on SPSS version 12.
Results: Seventy three patients with a mean age of 57.32 ± 13.87 years and range of 33-86 years presented with varying degrees of Fournier\'s gangrene. Of the total population, 67 (91.78%) were males and 6(8.213%) were females. Fifty nine (80.82%) patients had one or the other co-morbidity with maximum number (n=44, 60.2%) having diabetes mellitus. State of diabetes control was found to be an important prognostic factor. A source of infection was identified in skin, ano-rectal and perineal regions in 42 (57.53%) patients. Thirteen (17.80%) patients died despite aggressive conservative or surgical treatment.
Conclusion: Fournier\'s gangrene continues to be a lethal disease despite overall improvement in the antibiotic spectrum and surgical techniques. Diabetes remains the most important prognostic factor in the outcome of disease (JPMA 60:617; 2009).
Introduction
Fournier\'s gangrene is considered a threat due to its aggressiveness and ugly tendency to spread. Although rare, it is considered a potentially lethal disease due to its tendency to extend rapidly. It usually has a fulminant course if not treated aggressively. It is no longer considered an idiopathic disease as an infective source can often be found.1 It mainly affects the perineal region, genitals and the abdominal wall. There is a consensus that an aggressive medical treatment and extensive surgical debridement with colostomy, cystostomy, when necessary should be undertaken.2,3
Despite improved treatment with introduction of newer broad spectrum antibiotics, the reported mortality remains high.4-9 The organisms isolated range from bacteroids fragilis and E coli to Pseudomonas and clostridia, pepto streptococcus and streptococcus.10,11 The treatment options include conservative treatment comprising broad spectrum antibiotics and wound care while surgery remains the mainstay of the treatment and comprises repeated debridement of the dead tissue with sterile dressings. We report our experience of presentation, management and outcome of patients with Fournier\'s gangrene in our unit.
Methods
A prospective descriptive analysis of 73 diagnosed patients of Fournier\'s gangrene is done who were admitted and treated in surgical unit of a public sector university over a span of 8 years. All study subjects were admitted through casualty with necrotizing fasciitis and involvement of different areas of the body with varying proportions. After immediate resuscitation and preliminary investigations, patients were treated either conservatively by intra - venous antibiotics, cardio-pulmonary, nutritional and fluid support or surgically by repeated aggressive wound debridement under anaesthesia. An HbA1C was done in all patients who either had a history of diabetes mellitus or had blood sugar > 200mg% at arrival in the hospital. An HbA1C > 7 was considered uncontrolled diabetes while values lower than this were considered as controlled diabetes mellitus. Prior to institution of treatment, a culture of necrotic tissue was obtained in all patients which revealed Staphyloccoci and E.coli in majority of patients.
The variables studied included pattern of the disease, different modalities of treatment offered, response and outcome of the management in terms of morbidity and mortality. The statistical analysis of the data was done on SPSS version 12.
Results
Seventy three patients with a mean age of 53.16 ± 13.8 (range 33-86 years). There were 06 (8.1%) females and (n=67, 91.6%) males. There was an associated medical problem in 59 patients as shown in Table-1.
Status of the diabetes control seems to be an important prognostic factor. Diabetes was poorly controlled in majority of our study subjects as determined by HbA1C values. The personal hygiene of majority of patients was invariably poor. Of the total patients, 11 (14.9%) were homeless. Thorough examination of the patients revealed a septic focus in 49 (67.12%) patients in the perianal area, genitalia and on perineal skin. In 24 (32.8%) patients no septic focus could be identified. The area involved extended from genitals to whole abdomen, buttocks and back especially in patients with co-existent diabetes and renal failure. In 32 (43.8%) patients there was involvement of perineal region with an extension of the fasciitis to anterior abdominal wall, both flanks and even up to xiphoid process in few cases. Repeated excisions under anaesthesia was carried out in these patients with fulminating infection. Of these, 7(22%) patients had sufficient tissue loss and needed skin grafting after the infection was brought under control and wound was healthy looking.
In 22 (29.7%) patients the infection was localized to genitalia and /or perianal region. These patients were treated by intravenous antibiotics, I/V fluids and repeated de-sloughing and sterile surgical dressings.
Conservative treatment with repeated surgical dressings was found curative in 07 (31.8%) patients and in remaining patients we had to perform repeated excisions. The most effective antibiotics in terms of outcome included C-Penicillin and Metronidazole. The average hospital stay was 32 ± 08 days .Of the total patients treated, 13 (17.80%) patients succumbed to death despite aggressive treatment while 60 (81.8%) patients recovered completely and were discharged after an average time of 4.5 weeks. The mortality rate was highest in uncontrolled diabetics as shown in Table-2.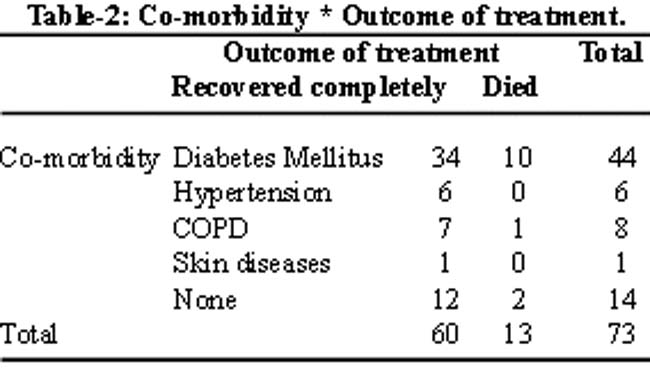
Discussion
First described by Fournier, the genital necrotizing fasciitis remains an uncommon but potentially a lethal disease with an alarmingly high mortality.12 The infection has an ugly tendency to spread and involve an extensive surface area if untreated, culminating in death. We report our experience of managing 73 consecutive patients of Fournier\'s gangrene with varying proportion of involvement of body surface area. The mean age of our study population coincides with other studies,10,13,14 although no age is immune from this disease.13 The course of disease is found to be very fulminant and aggressive in patients with associated diabetes mellitus. This is in accordance with the observation of many other authors who consider diabetes mellitus as one of the major outcome determinant of the treatment of this disease.15-17 Jong JH et al18 and Alan AL et al,19 however claim that diabetes mellitus is not related to the prognosis of the disease. An idiopathic variety of the disease was common in the past but it no longer carries this label. A septic focus was found in 54 patients in this study conforming to the results of other similar reports.20 The commonest underlying cause is found to be genitourinary (n=28) while colorectal origin was found in 07 patients. This is in contrast to many other similar reports claiming colorectal origin as the commonest underlying cause.21 A complete surgical excision of all dead tissue under anaesthesia gave excellent results in our study. This approach was the mainstay of treatment by many other authors.22,23
The average hospital stay in our study conforms with the results of many similar studies.4,7,17,24 This study showed an overall mortality of 18% of which most of the patients had uncontrolled diabetes mellitus. This significant finding is in line with the results of many similar reports from the west.25
The association of diabetes and urological problems observed in our study has been testified by literature from the west. The prognostic factors seem to be alike in most of the studies.
Conclusion
Fournier\'s gangrene, although rare, is potentially a lethal disease. Co-morbidities, especially diabetes mellitus increase the mortality manifold. Repeated surgical excisions and debridement with broad spectrum antibiotic provided good results.
References
1.Paty R, Smith AD. Gangrene and Fournier\'s gangrene. Urol clin North Am 1992; 19: 149-62.
2.Hejase MJ, Simonin JE, Bihrle R, Coogan CL. Genital fourniers gangrene: experience with 38 patients. Urology 1996; 47: 734-9.
3.Korhonen K. Hyperbaric oxygen therapy in acute necrotizing infections. With a special reference to the effects on tissue gas tension. Ann Chir Gynaecol 2000; Suppl 204: 7-36.
4.Spirnak JP, Resnik ML, Hampel N, Persky L. Fournier\'s gangrene: report of 20 patients. J Urol 1984; 131: 289-91.
5.Basoglu M, Gul O, Yildiqan I, Balik AA, Ozbey I, Oren D. Fournier\'s gangrene: review of fifteen cases. Am J Surg 1997; 63: 1019-21.
6.Basoglu M, Ozbey I, Atamanalp SS, Yildirqan MI, Aydinli B, Polat O, et al. Management of Fournier\'s gangrene: review of 45 cases. Surg Today 2007; 37: 558-63.
7.Geraci G, Pisello F, Lupo F, Cajozzo M, Scium C, Modica G. [Fournier\'s gangrene: case report and review of recent literature] Ann Ital Chir 2004; 75: 97-106.
8.Kuo CF, Wanq WS, Lee CM, Liu CP, Tseng HK. Fournier\'s gangrene: ten -year experience in a medical centre in northern Taiwan. J Microbiol Immunol Infect 2007; 40: 500-6.
9.Laucks SS 2nd. Fournier\'s gangrene. Surg Clin North Am 1994; 74: 1339-52.
10.Frezza EE, Atlas I. Minimal debridement in the treatment of Fournier\'s gangrene. Am Surg1999; 65: 1031-4.
11.Efem SE. The features and aetiology of Fournier\'s gangrene. Postgrad Med J 1994; 70: 568-71.
12.Grzybowski A. A short history of Fournier\'s gangrene. Arch Dermatol 2009; 145: 182.
13.Xeropotamos NS, Nousias VE, Kappas AM. Fournier\'s gangrene: diagnostic approach and therapeutic challenge. Eur J Surg 2002; 168: 91-5.
14.Hejase MJ, Simonin JE, Bihrle R, Coogan CL. Genital Fournier\'s gangrene: experience with 38 patients. Urology 1996; 47: 734-9.
15.Corman JM, Moody JA, Aronson WJ. Fournier\'s gangrene in a modern surgical setting: improved survival with aggressive management. BJU Intl 1999; 84: 85-8.
16.Diettrich NA, Mason JH. Fournier\'s gangrene. A general surgery problem. World J Surg 1983; 7: 288-94.
17.Korkut M, Icoz G, Dayangac M, Akgun E, Yeniay L, Erdogan O, et al. Outcome analysis in patients with Fournier\'s gangrene: report of 45 cases. Dis Colon Rectum 2003; 46: 649-52.
18.Jeong HJ, Park SC, Seo IY, Rim JS. Prognostic factors in Fournier gangrene. Intl J Urol 2005; 12: 1041-4.
19.Nisbet AA, Thompson IM. Impact of diabetes mellitus on the presentation and outcome of Fournier\'s gangrene. Urology 2002; 60: 775-9.
20.Di Falcol G, Guccionel C, D\'Annibalel A, Ronsisvallel S, Lavezzo P, Fregonese D, et al. Fournier\'s gangrene following a perineal abscess. Dis Colon Rectum 1986; 29: 582-5.
21.Stephen BJ, Lathrop JC, Rice WT, Gruenberg JC. Fournier\'s gangrene: historic (1764-1978) versus contemporary (1979-1988) differences in etiology and clinical importance. Am Surg 1993; 59: 149-54.
22.Picramenos D, Deliveliotis C, Macrichoritis K, Alexopoulou K, Kostakopoulos A, Dimopoulos C. [Fourniers gangrene: etiology, treatment, and complications]. Prog Urol 1995; 5: 701-5.
23.Kotrappa KS, Bansal RS, Amin NM. Necrotizing fasciitis. Am Fam Physicians 1996; 53: 1691-6.
24.Bahlmann JC, Fourie IJ, Arndt TC. Fourniers gangrene: necrotizing fasciitis of the male genitalia. Br j Urol 1983; 55: 85-8.
25.Wolach MD, McDermott JP, Stone AR, deVere White RW. Treatment and complications of Fourniers gangrene. Br J Urol 1989; 64: 310-4.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: