
Ahmad Usaid Qureshi ( Department of Paediatric Medicine, Children's Hospital, Institute of Child Health. Lahore, Pakistan. )
Agha Shabbir Ali ( Department of Paediatric Medicine, Lahore General Hospital, Post Graduate Medical Institute, Lahore, Pakistan. )
Arifa Hafeez ( Department of Developmental Paediatrics, Children's Hospital, Institute of Child Health. Lahore, Pakistan. )
Tahir Masood Ahmad ( Department of Paediatric Medicine, Children's Hospital, Institute of Child Health. Lahore, Pakistan. )
August 2010, Volume 60, Issue 8
Original Article
Abstract
Objectives: To compare the performance of paediatric medicine residents following a regular 6 hour and an extended 24 hour call and their own insight into their performance following each duty.
Method: The study was conducted at The Children\'s Hospital, Lahore, from September 2007 to November, 2008. All tasks were performed twice, after 6 hour call and 24 hour long call, evaluating Reaction timer, Concentration test, Number Connection Test, State Trait Anger Anxiety Inventory (STAXI) response for trait anger and modified Wechsler Memory Scale inventory (WMS-R) for cognitive performance. Likert\'s self assessment tool was used for both set of performances.
Result: Thirty two paediatric medicine residents (male 53.1%; female 46.9%) were enrolled in the study with identical duty structure performing 74 hours per week with mean age of 27.53 ± 0.32 years and mean experience of 3.69 ± 0.32 years. There was significant deterioration in both verbal recall and logic memory (mean difference in score of 1.81 (95% C.I 1.25-2.37, p<0.001). Concentration test also showed significantly fewer responses (24 hour mean 239.56, 95% C.I. 228-251.13) vs (6 hour mean 258.94, 95% C.I. 247.42-270.46) in 5 minutes, p<0.001. Reaction time, vigilance and hand eye coordination was significantly affected after an extended call, p<0.001. Number of lapses in attention also rose significantly, p<0.001. STAXI response showed significant increase in anger scores, p=0.001. Despite the significantly poor performance, the residents could not appreciate the deterioration in their performance with Likert\'s self assessment score that differed only by 0.63 (95% CI -0.12-1.37), p=0.1. None of the other factors studied correlated with deterioration in performance of any specific task except the length of duty hours.
Conclusion: Continuous long stretch of duty causes significant deterioration in cognitive and behavioural status of residents. More importantly, the residents themselves are unable to appreciate this deterioration. Residents must be made aware of this deterioration as there is a higher risk of medical errors and bad judgments, risking patient safety (JPMA 60:644; 2010).
Introduction
Long duty hours of resident doctors have been a cause of concern for a long time. Following an extended call, the consecutive duty stretches up to 30 or more hours during the residency. Long duty hours, continuous stretch of duty and burden of work all contribute to the deterioration in concentration, cognition and behaviour of the residents. The frequency of errors has also been suggested to increase with the rigorous schedule.1
The research in cognitive and behavioural deterioration has led to varied conclusions in the past. Most of the recent studies, however show considerable effect on mood, cognitive skills and professional accuracy due to extended work hours. Deterioration in simulated performance of physicians following a heavy long call has been comparable to the performance by physicians under the effect of 0.4 mg/dl alcohol. Work hour restrictions (< 80 hours per week) have been implemented in USA since 2002.2 Similar initiatives have been taken in the UK, Europe and Australia. After the implementation of restrictions, the residents from these settings have reported improvement in mood, self esteem and behaviour.
Serious concerns still loom over the residency programme where conventional thinking suggests that decreased work hours would reduce the exposure of training resident to number of patients. It also decreases the number of procedures performed by the resident questioning the attainment of professional competence for the specific procedures. Others have argued that decreased burden of work may allow more concentrating ability to the residents attaining competence in fewer number of procedures performed. The argument is also supported by evidence of decreased errors with lesser burden at work. Therefore, evaluation is also necessary to limit the risks to patients associated with consecutive long hours at work.3
The exact cause of the deterioration remains questionable. Whether chronic sleep deprivation due to long hours per week or acute sleep loss due to consecutive working hours at single stretch pose the most adverse effect remains to be defined. Unlike most studies, where overall work hours in a week were considered, effects of extended work hours at a stretch have not been studied sufficiently. The recent works do point out more detrimental effects on cognitive and behavioural status of resident doctors due to extended single stretch duty.2 In this study, the effect of consecutive extended hours on call were studied in detail, evaluating the deterioration in reaction time, concentration, memory and behaviour in Paediatric medicine residents following a routine 6 hour duty and a 24 hour extended call.
Subjects and Methods
The comparative within subject cross-sectional study was conducted at The Children\'s Hospital, Institute of Child Health, Lahore, Pakistan from September 2007 to November 2008. Possible participants included all paediatric medicine residents who had at least one year experience in the relevant field and had worked for at least one month in their present ward to minimize the effect of inexperience and new work setup. Study was conducted at a single centre only in order to minimize the confounding effects of different working environments. Work routine included an extended call every fourth day, dealing with indoor patients including a high dependency unit. Out of 49 possible participants, 38 residents volunteered. A sleep log was provided to confirm no participant was having chronic sleep deprivation and a self select sleep schedule allowing at least 8 hours uninterrupted sleep on all nights other than the extended call nights was followed. The sleep log was provided to all participants eight days prior to their first evaluation to document self select sleep schedule. Five residents were excluded as they were performing additional duties elsewhere and chronic sleep deprivation could not be ruled out. One resident, taking mood stabilizing medication, was also excluded. All tests were explained to participants a week prior to evaluation to limit the effect of inexperience with the tasks. The participants were not informed about the exact objective of the study to limit bias on behalf of the residents while attempting the tasks. The participants were restrained from taking caffeine or any other CNS stimulant at least 6 hours prior to the evaluation.4 Evaluations were performed by a clinical psychologist (Author AH) and senior registrar (Author AUQ) to remove observer bias. Study was approved by the Institutional Review Board and Medical Ethics Committee, Children\'s Hospital, Lahore.
Total number of patients under direct supervision and number of sick patients requiring frequent monitoring during the calls were recorded. Total number of procedures performed, including endotracheal intubations, intravenous access, chest intubations and various routine procedures were recorded. The performance tests included Standardized Number Connection Test A and B; recording mean performance time for vigilance and hand-eye coordination, performed twice in each set of tasks.5 Reaction time, through computer generated programme recording response to a visual stimulus (red spot turning to green) in milliseconds appearing at 2 to 10 seconds random delays for 5 minutes duration recorded mean response time and number of lapses in response (Lapse was defined as an extremely long reaction time <500 milliseconds or a complete failure to respond to stimuli).6 Concentration test, calculating number of correct responses to stimuli appearing on a computer generated programme in 5 minutes (A dot appearing randomly across a 10 x10 cm area on monitor screen), evaluated sustained attention and Modified W. Memory scale (WMS-R) evaluation was carried out for immediate response (IR) and delayed response (DR) to set of words and story passage verbally communicated to participants in beginning of the test for evaluating logic memory and verbal recall.7,8 STAXI immediate response (Trait Anger) was used to evaluate anger intensity in participants for behavioural changes.9 Trait Anger evaluates the overall behavioural pattern over 24 hour duration. State Anger was not considered as it represents the momentary state of behaviour and is affected severely with immediate preceding events prior to the evaluation and cannot represent the long term behavioural state of the person.10 Likert\'s Scale for self assessment of the participants including 7 point Performance Assessment, (1- extremely good, to 4- fair, to 7- extremely poor) and 4 point Effort Assessment (1- little effort required for task to 4- extreme effort)2,7 were carried out. The whole battery of tasks was performed twice: once after regular 6 hour call and then post-24 hour long call (around 24-26 hour on call depending upon availability of the resident for the test). Data was analyzed through SPSS v.14 (SPSS Inc. Chicago, IL.). Chi squared test was used for test of significance (two sided). Correlations were established using Pearson\'s R or Spearman correlation as applicable, with level of significance taken as p < 0.05.
Results
Thirty two paediatric medicine resident doctors (male 17, 53.1%; female 15, 46.9%) were enrolled in the study. Twenty three doctors were doing fellowship while nine having membership training. Their duties however, had identical structure and similar responsibilities. All the individuals were performing duties 74 hours per week and none was involved in any other part time job. The resident doctors were 25-33 years old (mean 27.53 ± 0.32 years) (Table-1).
Age difference was not significant between male and female residents (p=0.1). The age difference was also not significant between doctors in the two residency programmes (p=0.56). The experience of resident doctors after graduation ranged between 2-9 years (mean 3.69 ± 0.32 years) (Table-2).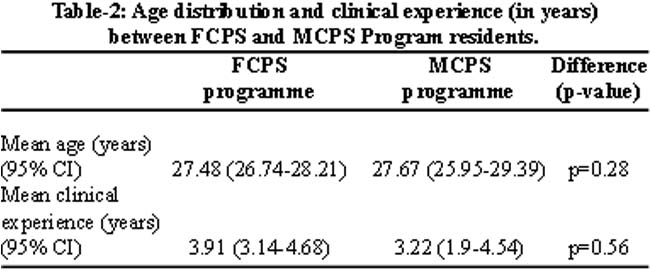
Clinical experience of the residents did not significantly differ with either gender (p=0.28) or residency programme (p=0.05). The residents looked after fourteen patients (95% C.I. 13.56-15.56) during a 6 hour duty with one sick patient requiring intensive monitoring on average. They were responsible for 55 patients (95% C.I. 50.23-59.84) during a 24 hour duty with an average of five sick patients. All participants had significantly less sleep hours during the extended call, p<0.01.
Residents performed one procedure (95% C.I. 0.61-1.39) during 6 hours duty and five procedures (95% C.I. 3.0-6.6) during 24 hours call.
WMS memory evaluation using a story showed a decrease in ability to retain short term memory after 24 hour call by score of 1.81 (95% C.I 1.25-2.37), significantly lower than after a 6 hour duty (p<0.001). WMS memory evaluation using pair of words also showed decrease in scores for both immediate (mean 1.28, 95% C.I. 0.86-1.7) and delayed responses (mean 1.2, 95% C.I. 0.79-1.6) after a 24 hours call. The response score was significantly lower after 24 hours call than after 6 hours call (p<0.001).
Number connection test performed by the residents was significantly slower after 24 hours call (mean 37.63 seconds, 95% C.I. 33.47-41.78 seconds) than 6 hours call (mean 28.29 seconds, 95% C.I 25.41-31.17 seconds), p<0.001. Concentration test showed significantly fewer responses after 24 hours duty (mean 239.56, 95% C.I. 228-251.13) than 6 hour duty (mean 258.94, 95% C.I. 247.42-270.46) in 5 minutes, p<0.001. Reaction time was also significantly delayed among the residents after a 24 hours call. Reaction time determined after 6 hours call (mean 289.26 milliseconds, 95% C.I. 267.74-310.78 milliseconds) increased significantly when determined after 24 hours duty (mean 320.92 milliseconds, 95% C.I. 297.55-344.29 milliseconds), p<0.001. Number of lapses in concentration during the 5 minutes test also increased significantly. Mean difference of 3.69 lapses (95% CI 1.68-5.69) was found between the two performances, (p=0.001).
Mean STAXI response score after 24 hours duty (16.56, 95% CI 14.33 - 18.79) was significantly higher than score after 6 hours (12.69, 95%CI 11.54 - 13.83), p=0.001.
Despite the significantly poor performance in all fields including memory recall, concentration and reaction time, the residents could not appreciate the deterioration in performance as the Likert\'s self assessment score for performance only differed by 0.63 (95% CI -0.12-1.37), p=0.1. The residents while analyzing their performance did believe they had to put in extra efforts to complete the tasks after 24 hours call than 6 hours duty. The Likert\'s self assessment score for effort required to perform increased significantly by 1.22 (95% CI 0.43-2.01), p=0.004 (Table-3).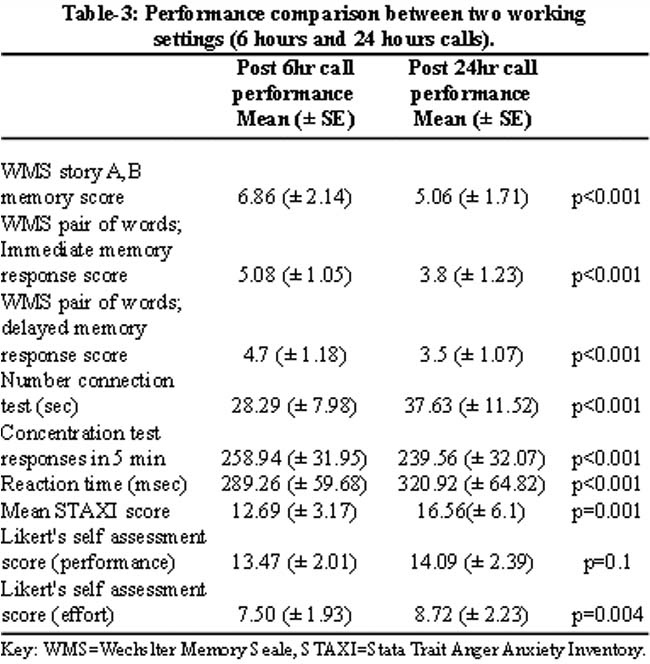
Only the duration of duty hours significantly correlated with deterioration of performance in all fields evaluated (p<0.001-0.008). Number of procedures performed only correlated significantly with deterioration in performance at sustained concentration tasks, p=0.004. Age and duration of clinical experience correlated significantly with lesser effort required for performing tasks, p=0.04. Both these factors however, did not correlate with deterioration in actual task performance, p=0.12-0.89. Fellowship residents had significantly better performance than membership residents in memory tasks and lesser lapses, p=0.01-0.03. However, there was no significant difference in rest of the tasks, p=0.2-0.9. None of the other factors studied including gender (p= 0.13-0.83), total number of patients under care or number of sick patients under care (p=0.67-0.87) correlated significantly with deterioration in performance of any specific task.
Discussion
Since the introduction of Accreditation Council for Graduate Medical Education (ACGME) time schedule and European Work Time Directive (EWTD), various studies have been conducted to evaluate the effects of these changes.11 The main aim of work hour restrictions was to improve quality of life of residents and at the same time limiting fatigue associated medical errors endangering patient care. The results of subjective assessment regarding the residents\' lives in some studies following new work routines have generated a mixed response. Most studies have shown an improvement in life of the residents.1,12 A few studies have reported a different response describing dissatisfaction and increased stress with new routine amongst residents.13 However, the residents included in assessment did long extended duties to save longer weekends and the aim of limiting stress of extended work hours could not take effect. Although they do not suffer from chronic sleep deprivation, acute sleep loss appeared as a major concern. Such routines result in same stress that occurred in previous work hour routines.14
Vigilance and hand-eye coordination are most sensitive to acute sleep loss as well as chronic partial sleep deprivation.2 Our study demonstrated significant deterioration in vigilance and hand-eye coordination in Concentration Test while randomly clicking on dots on monitor screen. Hand-eye coordination for Number Connection Test task was also significantly affected, taking mean 37.63 sec vs. 28.29 sec, p<0.001. Various other studies conducted previously on resident doctors and non resident professionals had similar results.15 Acute sleep loss affects performance significantly.4 Sustained attention also deteriorates with acute sleep deprivation especially at tasks requiring more than 3 minutes of attention. In our study, acute sleep loss was documented in all participants during extended calls. Sustained attention tested through Number Connection Test and Concentration Test was also significantly affected. Poor attention leads to medical errors in daily practice. We used a battery of tests that globally assessed all the traits required while performing a medical task instead of detecting medical errors because the stratification of minor or serious errors is very difficult. Moreover, they inherently include observer bias and objective results may become difficult to deduce. Various other studies showed similar deterioration in sustained attention and thereby increasing the number of medical errors after extended calls.166 One directly observed study documented 35.9% more errors after an extended work shift of more than 24 hours, p<0.001.17 These errors can very often result in dire consequences. Although previously anticipated, sleep loss resulting in errors is independent of type of resident\'s specialty. The deterioration extends to all fields including paediatrics, medicine and surgery. Twice the number of errors in ECG reporting, simulated laparoscopic procedures and percutaneous injuries have been documented following extended work hours.18 Tackling this acute sleep deprivation is tricky. Some experts have suggested inclusion of short naps during extended calls. Such efforts have resulted in further errors due to subsequent increased depth of sleep known as sleep inertia. As a result of sleep inertia, there has been documented increase in tendency to err on waking up.19 Another important cognitive function is the reaction time. It can severely affect the decision making and complex data processing.4 Reaction time was significantly increased in residents (mean 320.92 msec vs. 289.26 msec, p<0.001) in our study. Many other studies have shown a similar deterioration. Number of lapses was also significantly increased with a difference of 3.69 lapses in concentration every 5 minutes, p<0.001, compounding the odds for further medical errors. This finding was also similar to previous studies where significant attention failures have been documented after extended calls. These attention failures have resulted in grave medical errors and vehicle accidents.11 Memory recall is a significant cognitive function required during daily medical practice. Memory was severely affected in residents both in the area of logical memory and verbal recall, p<0.001. Both of these are very important in deducing inferences, decision making and carrying out orders. These findings were in agreement with various other studies evaluating memory functions.20
Behavioural status is also adversely affected due to extended work hours. It translates into worsening patient physician relationship. STAXI response was also significantly higher in residents, mean 16.56 vs. 12.69, p=0.001. Stress of extended duration of work was the most important factor increasing anger trait score. This finding was supported by previous studies including local data, showing improved patient care and better patient dealing with lesser work hours.21,22
The difference in performance was not affected by experience. This was in agreement with earlier studies suggesting that residents do not adapt to extended long calls with passing residency years.2 Performance was also not affected by number of procedures performed or the number of patients under direct care. It was against the proposed confounders by few studies.3 Fellowship training residents had significantly better performance in memory traits than membership trainees probably due to better cognitive abilities in the first place, p=0.01-0.03. The deterioration in memory was still significant in both groups after extended call. Self assessment scores were not significantly different as the residents could not assess their deteriorating performance with mean score difference 0.63, p=0.1. This was a real noticeable finding as the residents were not self aware of their cognitive and behavioural status deterioration which can increase risks while managing the sick patients. Self assessment has also been documented previously to be affected by fatigue and sleep loss.23 Residents could however feel that they had to put in significantly more effort while performing tasks after extended call.
Small sample size and single centre study although appear as a weak link in this study, it actually strengthens the assessment. A very strict selection criteria was applied to remove all confounding factors that may affect a person\'s performance in a given setting, unavoidably limiting the possible number of candidates and voluntary enrollment helped in maintaining a real life like working setup. Similarly, single centre setting removed all environmental factors like ambient temperature, working relations, different working setup and changing through specialties. Our study was randomized and performance was compared within subject, conducted over a whole year to minimize confounding factors like seasonal variations, experience, personality traits and other factors unrelated to the study. We believe the results are valid as the actual objective of study was not disclosed to the residents. Moreover, the self assessment consistently showed higher effort for comparable or poor performance. It is unlikely that residents could have titrated their performance so systematically.
Two important aspects of decreasing work hours of residents include possible lesser training for residents and poor patient care. Some studies had been suggesting that lesser work hours may hamper the training by lesser number of procedures.3 Although the number of procedures performed was significantly low, but these were mostly unsupervised emergency procedures, mostly endotracheal intubations. Various methods have been devised to improve the post call cognitive deterioration like using caffeine, ambient lights or controlling the circadian misalignment.24-26 All these efforts have met with little success and no widespread acceptance. Multiple transfers of care and discontinuity in care to the patients has been voiced but when compared to previous routines, there was only one extra transfer of care per day. To patients and their families, it may represent a marginal change.27 Cross coverage errors have been suggested to be minimized by sign out templates for uniform transfer of care with an extra hour of overlap between shifts with significant improvement. Recent audits have shown no deterioration in patient care since the implication of new work routines in terms of mortality rates,28 in fact, decreased work hours have shown to improve patient care.21
Conclusion
Our study clearly points out the deterioration of cognitive as well as behavioural functions of residents. All these traits have a direct effect on patient management and professional training. However, it was a single hospital study and the results may not be applicable in wider generalization. Multicentre trials are needed for further conformation of these findings. Taking into consideration the responsibility of optimal patient care services, it is imperative that residents must be made aware of post extended call impairment in their cognitive and behavioural skills as well as self assessment. It can be potential risk to the patients as the residents are unaware of their poor performance. Moreover, extended work hours may be reduced as much as feasible in a developing country like Pakistan so that residents may have improved professional training as well as quality of life.
References
1.Fletcher KE, Underwood W 3rd, Davis SQ, Mangrulkar RS, McMahon LF Jr, Saint S. Effects of work hour reduction on residents\' lives: a systematic review. JAMA 2005; 294: 1088-100.
2.Arnedt JT, Owens J, Crouch M, Stahl J, Carskadon MA. Neurobehavioral performance of residents after heavy night calls vs after alcohol ingestion. JAMA 2005; 294: 1025-33.
3.Dawson D, Zee P. Work hours and reducing fatigue-related risk: Good research vs good policy. JAMA 2005; 294: 1104-6.
4.Kamimori GH, Johnson D, Thorne D, Belenky G. Multiple caffeine doses maintain vigilance during early morning operations. Aviat Space Environ Med 2005; 76: 1046-50.
5.Saxena N, Bhatia M, Joshi YK, Garg PK, Tandon RK. Auditory P300 event-related potentials and number connection test for evaluation of subclinical hepatic encephalopathy in patients with cirrhosis of the liver: a follow-up study. J Gastroenterol Hepatol 2001; 16: 322-7.
6.Williams HL, Lubin A, Goodnow JJ. Impaired performance with acute sleep loss. Psychol-Mon Graphs 1959; 73: 1-26.
7.Wechsler D. Manual for the Wechsler Memory Scale-Revised. The Psychological Corporation, San Antonio (TX): 1987; 150 p.
8.Migoya J, Zimmerman SW, Golden CJ Abbreviated form of the Wechsler Memory Scale-III Faces subtest assessment. 2002; 9: 142-4.
9.Spielberger C., Ed. State-Trait-Anger-Expression-Inventory (STAXI). Odessa, FL Psychological Assessment Resources; 1988.
10.von Arb M, Gompper B, Meyer AH, Stutz EZ, Orgül S, Flammer J, et al. Relationship between gender role, anger expression, thermal discomfort and sleep onset latency in women. Biopsychosoc Med 2009; 3: 11.
11.Philibert I, Friedmann P, Williams WT. ACGME Work Group on Resident Duty Hours. Accreditation Council for Graduate Medical Education. New requirements for resident duty hours. JAMA 2002; 288: 1112-4.
12.Lockley SW, Cronin JW, Evans EE, Cade BE, Lee CJ, Landrigan CP, et al. Effect of reducing interns\' weekly work hours on sleep and attentional failures. N Engl J Med 2004; 351: 1829-37.
13.Grover K, Gatt M, MacFie J. The effect of the EWTD on surgical SpRs: a regional survey. Ann R Coll Surg Engl 2008; (Suppl) 90: 68-70.
14.Landrigan CP, Fahrenkopf AM, Lewin D, Sharek PJ, Barger LK, Eisner M, et al. Effects of the accreditation council for graduate medical education duty hour limits on sleep, work hours, and safety. Paediatrics 2008; 122: 250-8.
15.Bartel P, Offermeier W, Smith F, Becker P. Attention and working memory in resident anaesthetists after night duty: group and individual effects. Occup Environ Med 2004; 61: 167-70.
16.Kaushal R, Bates DW, Landrigan C, McKenna KJ, Clapp MD, Federico F, et al. Medication errors and adverse drug events in paediatric inpatients. JAMA 2001; 285: 2114-20.
17.Landrigan CP, Rothschild JM, Cronin JW, Kaushal R, Burdick E, Katz JT, et al. Effect of reducing interns\' work hours on serious medical errors in intensive care units. N Engl J Med 2004; 351: 1838-48.
18.Ayas NT, Barger LK, Cade BE, Hashimoto DM, Rosner B, Cronin JW, et al. Extended work duration and the risk of self-reported percutaneous injuries in interns. JAMA 2006; 296: 1055-62.
19.Dinges DF. Are you awake? Cognitive performance and reverie during the hypnopompic state. In: Bootzin R, Kihlstrom J, Schacter DL, Eds. Sleep and cognition. Washington, D.C.: American Psychological Association, 1990: 159-75.
20.Abikoff H, Alvir J, Hong G, Sukoff R, Orazio J, Solomon S, et al. Logical memory subtest of the Wechsler Memory Scale: age and education norms and alternate-form reliability of two scoring systems J Clin Exp Neuropsychol 1987; 9: 435-48.
21.Shanafelt TD, Bradley KA, Wipf JE, Back AL. Burnout and self-reported patient care in an internal medicine residency program. Ann Intern Med 2002; 136: 358-67.
22.Kasi PM, Khawar T, Khan FH, Kiani JG, Khan UZ, Khan HM, et al. Studying the association between postgraduate trainees\' work hours, stress and the use of maladaptive coping strategies. J Ayub Med Coll Abbottabad 2007; 19: 37-41.
23.Dorrian J, Lamond N, Dawson D. The ability to self-monitor performance when fatigued. J Sleep Res 2000; 9: 137-44.
24.Wyatt JK, Cajochen C, Ritz-De Cecco A, Czeisler CA, Dijk DJ. Low-dose repeated caffeine administration for circadian-phase dependent performance degradation during extended wakefulness. Sleep 2004; 27: 374-81.
25.Czeisler CA, Johnson MP, Duffy JF, Brown EN, Ronda JM, Kronauer RE. Exposure to bright light and darkness to treat physiologic maladaptation to night work. N Engl J Med 1990; 322: 1253-9.
26.Lockley SW, Brainard GC, Czeisler CA. High sensitivity of the human circadian melatonin rhythm to resetting by short wavelength light. J Clin Endocrinol Metab 2003; 88: 4502-5.
27.Goldman L, Fiebach NH. Hippocrates affirmed? Limiting residents\' work hours does no harm to patients. Ann Intern Med 2007; 147: 143-4.
28.Volpp KG, Rosen AK, Rosenbaum PR, Romano PS, Even-Shashan O, Wang Y, et al. Mortality among hospitalized Medicare beneficiaries in the first 2 years following ACGME resident duty hour reform. JAMA 2007; 298: 975-83.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: