
Zamir Butt ( Pakistan Institute of Medical Sciences (PIMS), Islamabad, Pakistan. )
Qurratulain Hyder ( Pakistan Institute of Medical Sciences (PIMS), Islamabad, Pakistan. )
August 2010, Volume 60, Issue 8
Original Article
Abstract
Objective: To determine the role of risk factors, which promote cholelithasis in Hepatic Cirrhosis (HC).
Methods: A prospective study was conducted on indoor cases with advanced HC. Outpatients with compensated Chronic Liver Disease were used as control. The subjects with history of cholecystectomy and diabetes mellitus were excluded from the study. Conventional ultrasound was used for the detection of gallstones, ascites and portal hypertension. Sonography also furnished pertinent information about the portal vein diameter, size of the spleen, gallbladder wall thickness and echogenecity of the liver.
Results: The number of registered cases was 206: (age: 30-85 years): 121 (58.7%) males and 85 (41.3%) females. Hepatitis C (HCV) was the cause of HC in 187 (90.88%) cases. Of 50 (24.30%) patients with detectable gallstones, 27(54.00%) were males. We observed correlation of several risk factors with cholelithasis in our patients (n=50): advanced age: mean 57.3 ± 9.7 years (100%); prolonged duration of HC: 3.5 years (100%); Child -Pughs\' class C: 34 (68%); increased thickness of gallbladder wall: 45 (90%); gross ascites: 39 (78%); splenic enlargement: 17.3cm (100%); increased portal vein diameter: 13.4mm (100%). The results were statistically significant when compared with the control group (p=<0,001).
Conclusion: Gallstones tend to occur more frequently in patients with decompensated CLD due to interaction of several risk factors in these patients (JPMA 60:641; 2010).
Introduction
HCV is the principal cause of Chronic Liver Disease (CLD) in the local population. The prevalence of gallstones in general population and Hepatic Carcinoma (HC) is reported as 10-15% and 23.3-31%, respectively.1-4 The association between HC and cholelithiasis was originally documented in autopsy studies.5 The gallstones in CLD are often incidental and warrant elective intervention in symptomatic patients. A controversy prevails about the pathogenesis of biliary stones in CLD.6-10 This study was undertaken to identify the relationship between the precipitating factors and occurrence of gallstones in HC.
Patients and Methods
The present study was conducted at PIMS (Department of Gastroenterology) between March-August, 2008. Indoor cases with decompensated CLD were enrolled for the study. The sample size was calculated using WHO sample size calculator where confidence level is 95%. Absolute precision: (d) =0.6 P (ref)3 = 26%; sample size: n= 206 (hospitalized cirrhotic patients) and sample technique: non probability and purposive. Closely matched outpatients with well compensated HC were used as controls. Patients with previous cholecystectomy and diabetes mellitus were excluded. All cases were subjected to clinical, biochemical and radiological evaluation. Transcutaneous abdominal ultrasound was performed using 3.5 MHZ device (model: Philips: MCMD-02AA). The computer programme SPSS Version 11 was used for statistical analysis. CHI-square and FISHER test were used for categorical variables. P-value <0.05 was considered to be statistically significant. Wall thickness >4 mm on ultrasound was interpreted as abnormal.
The diagnosis of HC was based on stigmata of CLD and increased echogenicity of the liver.
CLD was considered to be compensated if the patient had no evidence of ascites or metabolic decompensation.
CLD was regarded as decompensated if the subject presented with ascites &/or hepatic encephalopathy (i.e. altered sensorium, \'hepatic flap\', abnormal behaviour or deep coma).
Duration of HC: It was roughly estimated from Child-Pughs\' class and age of the patient.11
Bipolar length of the spleen >12cm on conventional ultrasound was considered as Splenomegaly.6
The diagnosis of portal hypertension was entertained if sonographic diameter of the portal vein exceeded 13mm.6
The measurements above 4 mm of gallbladder wall on ultrasound were taken as abnormal.6
Results
Of 206 subjects in the decompensated series, there were 121 (58.70%) males and 85 (41.30%) females (age: 30-85 years; mean age: 53.3 ± 9.9 years). The etiology of CLD in our patients included: HCV: 187 (90.80%); hepatitis B (HBV): 18 (8.70%); Wilsons\' disease: 1 (0.50%). They were placed in Child-Pughs\' class A: 34 (16.50%); B: 99 (48.10%); C: 73 (35.40%). The approximate duration of HC was 1-5 years. In the closely matched compensated series, there were 206 patients: 118 (53.30%) males and 88 (42.70%) females (age: 27-58 years; mean age: 44.0 ± 7.8 years). CLD in these subjects was due to HCV: 194 (94.0%); HBV: 12 (5.80%). All patients in the control group belonged to Child-Pughs\' class A and the duration of HC was 1-3 years (Table-1).
The sonographic findings in decompensated patients were (n=206): reduced size of the liver with coarse echotexture and irregular margins: 206 (100%); ascites: 196 (95.1%) cholelithiasis: 50 (24.30%); gallbladder wall thickness increased 84(40.80%) and normal 122 (59.20%). The measurements for splenic size and portal vein diameter were 9.0-18.6 cm and 9.0-20 mm, respectively. Sonography in the control group demonstrated (n=206): increased echogenecity of the liver: 206 (100%); ascites: 2 (1.0%); gallstones: 20 (9.7%); gallbladder wall thickness increased 12 (5.9%) and normal 194 (94.1%). Size of the spleen and portal vein diameter varied between 7-14 mm and 6-13 mm, respectively (Table-2).
In our patients with decompensated CLD and cholelithiasis (n=50), the presence of gallstones was significantly correlated with certain risk factors (p <0.001): advanced age (57.3 ± 9.5 years): 50 (100%); longer duration of HC (3.5 ± 1.0 years) 50 (100%); Child -Pughs\' class C: 34 (68%); splenic enlargement (17.3 ± 1.7cm): 50 (100%); dilatation of portal vein: (13.5 ± 1.4mm): 50 (100%); gross ascites: 39 (78%); increased gallbladder wall thickness: 45 (90%) (Table-3).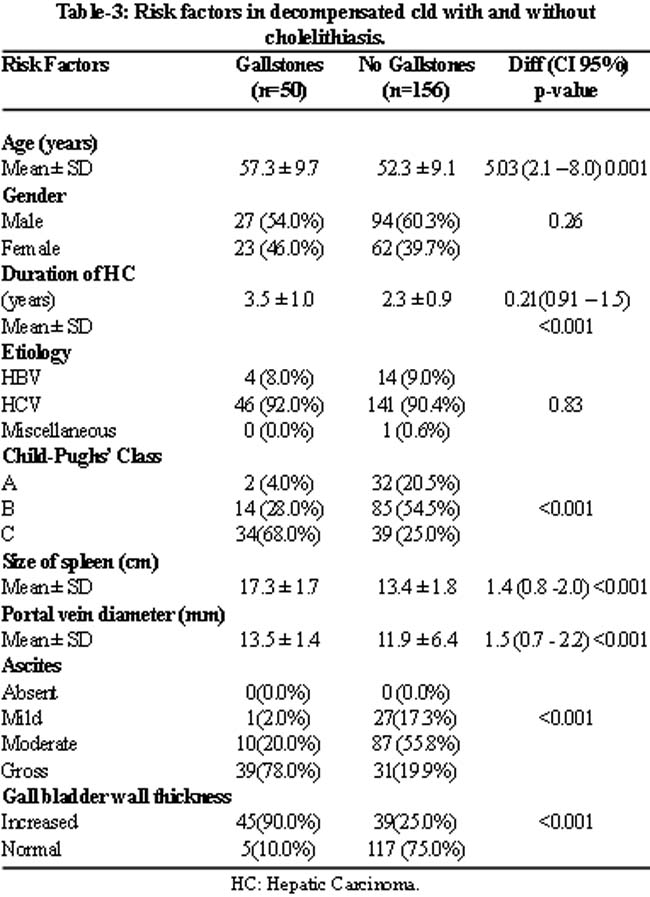
When compared with the compensated group (n=206), the statistics for risk factors were significantly different in subjects with decompensated CLD and gallstones (n=50): advanced age: >57 years vs <49 years; duration of HC: >3 years vs <1 year; Child-Pughs\' class: C vs A & B; portal vein diameter: >13mm vs <11mm; ascites: gross vs minimal to none; gallbladder wall thickness >4 mm vs <4mm.
Discussion
Based on our findings in the present study, the formation of gallstones in decompensated liver disease can be attributed to the interaction of several adverse factors. Naheed et al have reported a higher incidence of cholelithiasis in 100 patients with HC.4 Acalovschi et al also maintain that the incidence of gallstones is five times higher in decompensated HC.8 Conte and Silva et al augment our viewpoint that the prevailing risk factors account for high incidence of gallstones in decompensated CLD.3,7 These observations compare favourably with our results. According to Conte et al increased frequency of gallstones in CLD is not related to gender.3 However, the influence of gender on cholelithiasis is observed more often in general population, especially amongst females. The frequent occurrence of gallstones in fertile women is possibly due to excessive secretion of cholesterol into bile under the influence of estrogen.12 With decline in estrogen levels after menopause, the incidence of gallstones in women is significantly reduced.3,12 Cholelithiasis in our subjects above 50 years of age supports the inference by Zhang et al that advanced age is related with the genesis of gallstones in CLD. It is due to excessive secretion of cholesterol and low content of bile salts in hepatic bile. Moreover, there is decreased hepatic elimination of estrogen in elderly patients.3,6 Silva et al conclude that the age impacts cholelithiasis by increase in severity of the liver disease.7 In our practical experience, both HCV and HBV infections are generally acquired in childhood and hepatic decompensation occurs after 20-25 years.11 The majority of patients with gallstones in the present study belong to Child-Pughs\' class C. The difference in various risk factors in our decompensated and compensated groups is statistically significant.
According to Sarin et al, gallstones are twice as common in CLD with portal hypertension.13 Zhang et al state that portal hypertension is an important risk factor, which promotes cholelithiasis in decompensated CLD.6,14,15 It is due to prolonged congestion and increase in venous hydrostatic pressure, which results in oedema of the gallbladder.16 The latter may also exist in the absence of hypoalbuminaemia and ascites.6 Thickened gallbladder walls contribute to reduced contractility of the gallbladder.6,12,17 It is an important factor in the genesis of gallstones in such patients. Chawlaw et al attribute impaired emptying of gallbladder in decompensated CLD to autonomic neuropathy.18 Jin et al have found that cutting of the vagus nerve could inhibit contractility of gallbladder.19 We believe that non clearance of several toxic substances by the diseased liver in advanced CLD may add to autonomic neuropathy, gallbladder stasis and subsequent stone formation.
Conclusion
The higher incidence of cholelithasis in CLD appears to be associated with age, portal hypertension, gallbladder stasis and severity of the liver disease. Since these gallstones are usually asymptomatic, surgery should be avoided in such patients.
References
1.Almani SA, Memon AS, Memon AI, Shah I, Rahpoto Q, Solangi R. Cirrhosis of liver: Etiological factors, complications and prognosis. J Liaquat Uni Med Health Sci 2008; 7: 61-6.
2.Razi M, Nadia I, Qamer A, Omar I. Pattern of gallbladder disease in Pakistan. Pak J Med Sci 1999; 15: 109-12.
3.Conte D, Fraqulli M, Fornari F, Lodi L, Bodini P, Buscarini L. Close relation between cirrhosis and gallstones: Cross-sectional and longitudinal surgery. Arch inters Med 1999; 159: 49-52.
4.Naheed T, Akbar N. Frequency of gallstones in patients of liver cirrhosis; a study at Lahore. Pak J Med Sci 2004; 20: 215-8.
5.Bouchier IA. Postmortem study of the frequency of gallstones in patients with cirrhosis of liver. Gut 1969; 10: 705-10.
6.Zhang Y, Liu D, Ma Q, Dong C, Wei W, Chen W. Factors influencing the prevalence of gallstones in liver cirrhosis. J Gasroenterol Hepatol 2006; 21: 1455-8.
7.Silva MA, Wong T. Gallstones in chronic liver disease. J Gastrointest Surg 2005; 9: 739-46.
8.Ichiyanaqui C, Monge E, Huaman C, Flores C, Beteta O, Soto W. [Cholelithiasis in patients with liver cirrhosis]. Rev Gastroenterol Peru 1996; 16: 43-7.
9.Orozco H, Takahashi T, Mercado MA, Prado E, Boronda D. Long term evaluation asymptomatic cholelithiasis diagnosis during abdominal operation for variceal bleeding in patients with cirrhosis. Am J Surg 1994; 168: 232-4.
10.Acalovschi M, Blendea D. Risk factors for symptomatic gallstones in patients with liver cirrhosis; a case control study. Am J Gastroenter 2003; 98: 1856-60.
11.Rurtherford A, Dienstag JL. Viral Hepatitis in Greenberger N J, Blumberg RS, Burakoff R (editor). Current Diagnosis and Treatment. Delhi: Tata McGraw-Hill, 2009; 434-440.
12.Jaferrey DB, Sreenarasimhaiah J. Gallstone diseases in Feldman M, Friedman LS, Brandat LO (editor). Sleisenger and Fordtrans\' Gastrointestinal and Liver diseases. 8th ed. Philadelphia: WB Saunders, 2006; 1387-413.
13.Sarin SK, Guptun RC, Malhotra S. Increase frequency of gallstones in cirrhotic and non-cirrhotic portal hypertension. J Asso Physician India 2002; 50: 518-22.
14.Sohn BK, Hahim JS, Lee HL, Lee JS, Eun CS, Park JY, et al. Analysis of Risk Factors Affecting Gallstone Formation in Liver Cirrhosis. Korean J Gastroenterol 2001; 37: 443-7.
15.Acalovschi M, Badea R, Pascu M. Incidence of gallstones in liver cirrhosis. Am J Gastroenterol 2008; 134: 416-23.
16.Vijay HS, Patric SK. Portal hypertension and gastrointestinal bleeding in Feldman, Friedman, Brandt LO (editor) Sleisenger and Fordtrans\' Gastrointestinal and liver diseases. 8th ed. Philadelphia: WB Saunders, 2006; 1899-906.
17.Elzouki AN, Nilsson S, Nilssen P, Veibaan H, Simanaitis M, Lindgren S. The prevalence of gallstones in chronic liver disease is related to degree of liver dysfunction. Hepatogastroenterology 1999; 46: 2946-50.
18.Chawla A, Puthumana L, Thuluvath PJ. Autonomic dysfunction and cholelithiasis in patients with cirrhosis. Digestive Diseases Sciences 2004; 49: 17-24.
19.Jin H, Wu SD, Zhang F, Chen XY, Zhang GX. Gallbladder motility in patients with hepatic cirrhosis before and after azygous disconnection. World J Gastroenterol 2004; 10: 3230-3.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: