
Muhammad Khurram ( Department of Medicine, Holy Family Hospital, Rawalpindi.. )
Wajeeha Qayyum ( Department of Medicine, Holy Family Hospital, Rawalpindi.. )
Mohammad Umar ( Department of Medicine, Holy Family Hospital, Rawalpindi. )
Mohammad Jawad ( Department of Medicine, Physician, Ministry of Health, KSA.. )
Shumaila Mumtaz ( Department of Medicine, Holy Family Hospital, Rawalpindi. )
HamamTul Bushra Khaar ( Department of Medicine, Holy Family Hospital, Rawalpind. )
March 2016, Volume 66, Issue 3
Original Article
Abstract
Objective: To note ultrasonographic findings used for diagnosing plasma leakage in dengue haemorrhagic fever patients.
Methods: The observational retrospective study was conducted at the Holy Family Hospital, Rawalpindi and comprised records of patients with confirmed dengue infection who were screened for dengue haemorrhagic fever according to Dengue Expert Advisory Group criteria from July 1 to December 31, 2013. Each patient underwent ultrasonography for the detection of ascites, gall bladder wall thickness, pleural and/or pericardial effusion along with their quantification and localisation.
Results: Of the 240 patients, 166(69.2%) were men. The overall mean age was 28.9±12.4 years. Of the total, 215(89.5%) had ultrasonographic abnormalities, suggestive of plasma leakage. Quantification and localisation wise, mild abdominal ascites 68(47.2%), right pleural effusion 82(74.5%) and mild pleural effusion 98(89%) were commonly noted. None had pericardial effusion.
Conclusion: Mild ascites and mild right pleural effusion were the commonest pattern of ultrasonographic leak in dengue haemorrhagic fever patients.
Keywords: Dengue, Dengue haemorrhagic fever, Ultrasonography, Ascites, Pleural effusion. (JPMA 65: 260; 2015)
Introduction
Dengue fever (DF) is an important arthropod-borne viral disease.1,2 The incidence of dengue is on the rise all over the world.3 Over 2.5 billion people that make more than one-third of the world\\\'s population are at risk of dengue infection.3 Every year 50-100 million people suffer from dengue. Dengue haemorrhagic fever (DHF) is the more serious version of dengue infection.3,4 Up to 5% mortality is associated with DHF.2,5 Dengue infection is an important healthcare issue in Pakistani scenario. About 18,000 Pakistanis suffered from dengue infection in the year 2011 and almost 350 deaths were attributed to it.4,6
There are 4 serotypes (1-4) of dengue virus.7 Generally, first infection or primary infection is associated with DF, while reinfection with another serotype causes DHF.7 Plasma leakage differentiates DHF from DF.7-12 Diagnosis of plasma leakage can be made in a number of ways. These include haemoconcentration, presence of pleural or pericardial effusion, ascites or gall bladder wall thickness [GBWT], hypoproteinaemia, and hypocholestrolaemia in a suggestive clinical scenario.7-12 Of these, haemoconcentration is the most widely used criteria for confirming plasma leakage. A number of factors may affect these diagnostic criteria which include not frequently knowing baseline haematocrit (Hct), individual and racial differences in Hct, and effect of fluid administration and bleeding on Hct.13
In order to improve outcome in dengue infection, early diagnosis of plasma leakage and, thus, of DHF are important.14,15 Clinical and radiological examination for detection of ascites and pleural effusion can\\\'t diagnose leakage in initial stages.15 Ultrasound is a sensitive technique for the detection of minimal pleural effusion and ascites.13,16 It can help in diagnosing DHF much earlier.15 Rawalpindi faced dengue epidemic during 2013.17,18 During this epidemic, majority of DHF patients were treated at the Holy Family Hospital, Rawalpindi.6,17,18 This study was planned to note ultrasonographic (USG) findings used for diagnosing plasma leakage in patients managed with diagnosis of DHF. Additionally, DHF patients were compared in terms of severity of illness and the diagnostic basis of leak.
Patients and Methods
The observational study was conducted at the Medical Unit of Holy Family Hospital, Rawalpindi, from July 1 to December 31, 2013, after approval from the Departmental Ethics Committee. All patients with confirmed dengue infection were screened for DHF. These patients had febrile illness of 2-10 days, leucocyte count <3000 mm3, platelets count <100000/mm3, or rapidly falling platelets, and positive dengue serology.8,9 Serological evidence of dengue infection was based on positive nonstructural protein 1(NS1) antigen or dengue specific immunoglobulin M (IgM), or >4 time rise in paired dengue-specific IgG levels if IgM and NS1 were negative.8-11
Each patient underwent clinical evaluation and investigations for screening of DHF diagnosis based on Dengue Expert Advisory Group (DEAG) criteria according to which DHF is characterised by plasma leakage as shown by haemoconcentration (an increase in Hct >20% above average for age or decrease in Hct >20% of baseline following fluid replacement therapy, pleural effusion, ascites, or hypoproteinaemia.8-11 Repetitive clinical examinations, laboratory investigations, and USG evaluations were conducted in this regard. Patients with diagnosis of DHF were finally included after their or their families\\\' informed consent.
Regarding USG, standard abdominal and chest examinations were performed (Honda Electronics, Convex Scanner HS-2000) with 3.75MHz probe for detection of plasma leakage by a trained ultrasonographer. USG findings suggestive of plasma leakage included detection of one or more of the following; pleural effusion, ascites, GBWT>3mm19 and pericardial effusion. Pleural effusions if present were further categorised into right, left, bilateral, mild, moderate and large. Ascites if present was categorised into pelvic only, and abdominopelvic. Abdominopelvic ascites were further categorised into mild, moderate and massive ascites.
A specifically-designed proforma was used to note USG findings along with age, gender, diagnostic bases (Hct-based, USG-based), disease severity (DHF or dengue shock syndrome [DSS])13,15 and outcome (recovered or expired).
Using SPSS 19, frequencies and percentages were calculated for gender, DHF diagnostic basis, disease severity, outcome and USG abnormalities. Mean ± standard deviation were noted for age. Sensitivity analysis of USG-based DHF diagnosis compared to gold standard Hct-based diagnosis was also carried out.
Results
Out of 811 patients managed with diagnosis of confirmed dengue infection, 255(31.4%) met the DHF criteria. Of them, 240(94%) patients comprised the study sample as USG findings of 15(6%) patients were incomplete or missing. Of the 240 subjects, 166(69.2%) were men. Overall mean age was 28.9±12.4 years; 229(95.4%) were diagnosed as DHF and 11(4.6%) as DSS; 221(92.1%) patients improved and were discharged; 8(3.3%expired; and outcome of 11(4.6%) patients was not known as they were discharged on request or left against medical advice.
Besides, 205(85.4%) were diagnosed DHF based on combined Hct and USG findings, 25(10.4%) on Hct findings alone, and 10(4.2%) on USG findings alone. Further, 230(95.3%) patients were diagnosed DHF based on Hct findings and 215(89.5%) on USG abnormalities suggestive of plasma leakage. USG-based DHF diagnosis had 93.48% sensitivity, 100% specificity, 100% positive predictive value (PPV), and 97.42% negative predictive value (NPV) compared to Hct-based diagnosis.
Mean age of patients with USG leakage was less (28.1±11.4 years) compared to patients without it (36.4±18 years). Gender and outcome wise, patients with and without USG leakage were comparable. Details in this regard are given in (Table-1).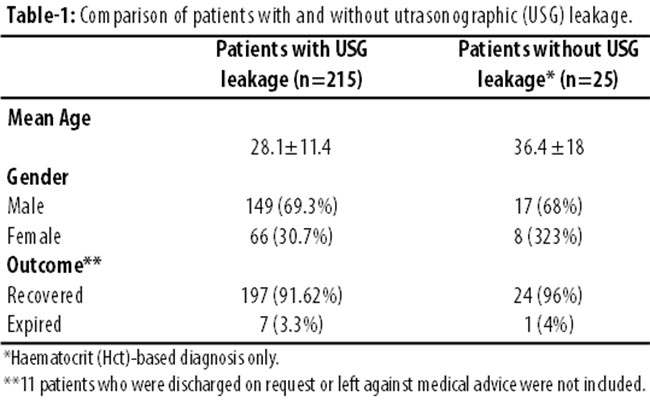
Ascites 144(66.9%) was the most frequently noted USG finding followed by pleural effusion 110(51.1%), and GBWT51(23.7%) (Table-2).
Besides, 57(26.5%) patients had combined ascites and pleural effusion; 27(12.5%) had combined ascites and GBWT; 13(6%) had combined pleural effusion and GBWT; and 7(3.2%) had combined ascites, pleural effusion and GBWT.
In terms of findings suggestive of USG leakage, 144(61.6%) DHF patients had ascites compared to 4(36.3%) DSS patients. Pleural effusion and GBWT were noted in 103(45%) and 50(21.8%) DHF patients compared to 7(63.7%) and 1(9.1%) DSS patients (Table-3).
Discussion
Although a number of studies have focused on USG findings in DHF patients, but our study stands distinct as it focuses on regional dengue epidemic, comparatively much higher number of patients are included, and GBWT was included in the analysis of patients with USG leakage. We noted USG findings suggestive of plasma leakage in 89.5% DHF patients. USG leakage in the form of pleural effusion, ascites and GBWT has been noted in up to 100% patients with DHF.20 A study noted that 91.42% (32/35) DHF paediatric patients had USG findings suggestive of plasma leakage.21 In a study 72.72% (48/66) DHF patients who were 14 or more years of age had USG evidence of leakage.22 In a study focusing natural history of plasma leakage in DHF, 76% patients (16/21) had USG plasma leakage.23 In DHF, USG-based detection of leak is considered to have high sensitivity and predictive value.21,22,24 Our results are comparable in this regard.
Ascites was the most common USG finding in our DHF patients. Variable results have been noted in studies regarding this. A study on sonographic findings of adults with grade III DHF found that only 15% patients had ascites.24 It included 40 patients. In another study, 92% (11/12) patients had ascites.25 One study noted ascites in 91.4% (32/35) DHF patients.21 In one study, sequential ultrasonography showed ascites in 52% of 21 DHF patients.23 In another study 36.3% (24/66) patients had USG evidence of ascites.22 Mild abdominal ascites was most frequently, and massive abdominal ascites was least frequently noted in our study. In some studies mild and in other moderate to massive ascites have been noted in DHF patients.24,25
Pleural effusion has been considered a more reliable marker of plasma leakage compared to ascites in DHF patients.19,24 In a study, 79% of 50 patients with DHF had pleural effusion on ultrasonography.26 In an Indian study, 88.5% of 35 DHF patients had pleural effusion.21 In a study from Thailand, 62% of 21 DHF patients had pleural effusion.23 In three other studies,53, 82 and 97.9% of DHF patients had pleural effusion respectively.24,25,27 In our study pleural effusions were less frequently noted.
Pleural effusions in dengue infection are generally exudative, mild and bilateral.28 Right-sided pleural effusion has been considered a sensitive marker of plasma leak in early period of DHF.16 In a Pakistani study that included 159 DHF patients, right-sided pleural effusion was noted in 12.5%.29 Majority of our patients had mild and right-sided pleural effusion.
GBWT is considered an important ultrasonographic finding suggestive of plasma leakage in DHF patients. In a Pakistani study conducted in Faisalabad, GBWT was noted in 86.6% of mild DHF and 100% of severe DHF patients.30 According to a study from Taiwan, GBWT is the most frequently seen USG pattern of plasma leakage.31 In a study from India, GBWT was noted in all of the 20 DHF cases.14 In Indonesia, a study noted GBWT in 72.7% of 66 DHF patients.22 Frequency of GBWT in our patients is comparatively very less i.e., 23.7%.
Plasma leakage features in combination: ascites in combination with pleural effusion; and ascites, pleural effusion and GBWT etc. This factor has not been focussed exclusively in various studies. In one study 40.9% patients had combined ascites and pleural effusion.22 In this context the commonest combinations in our study were ascites with pleural effusion, and ascites with GBWT.
Plasma leakage in DHF patients can cause pericardial effusion as well. Pericardial involvement in dengue infection is considered uncommon unless disease is severe.32 In a Bangladeshi study, 6% of the dengue patients had pericardial effusion.33 10% dengue infected patients (16/158) had pericardial effusion in a Pakistani study.34 Interestingly, we did not note pericardial effusion in any patient even with severe disease.
Severity of plasma leakage in DHF patients correlate with the severity of disease.19,30 In an Indonesian study, 34% patients with mild DHF, and 95% with severe DHF had ascites on ultrasound examination.25 Pleural effusions were noted in 30% patients with mild and 95% patients with severe DHF in the same study.25 All (100%) patients with severe DHF and 86.6% patients with mild DHF had GBWT in a Pakistani study from Faisalabad.34 Our results are different in this regard. Percentage wise, compared to DHF patients, our DSS patients had less ascites and GBWT. Similarly, pleural effusions were more frequently noted in DHF patients. These differences were, however, statistically insignificant. We also compared DHF patients with and without USG evidence of plasma leak. Mean age of patients with USG plasma leakage was less. Gender and outcome wise, no remarkable difference was noted between patients with and without USG leakage.
Large sample representing epidemic-hit population and results comparable with other studies are important positive points about the external validity of our study. It should, however, be noted that not all DHF patients during the epidemic were treated at the hospital where the study was conducted, and the study sample represents mainly adults. Additionally, the 2013 Rawalpindi dengue epidemic was caused by Den-2 virus.35
Conclusion
Ultrasound was found to be an important tool for diagnosing plasma leakage in DHF patients. Ascites and pleural effusion were most frequently noted pattern of USG leakage. Mild abdominal ascites, and mild right-sided effusion were the commonest patterns of these. GBWT was less frequently noted, while pericardial effusion was not noted. USG and Hct changes had comparable results for leak evaluation. DHF and DSS patients did not differ in terms of presence or absence of ascites, pleural effusion and GBWT. Mean age of DHF patients with USG leakage was less compared to patients without USG leakage.
Acknowledgements
We are grateful to the Dengue Team, Administration and staff of Medical & Allied Departments of the Holy Family Hospital, Rawalpindi, for their support.
References
1. Venkata Sai PM, Dev B, Krishnan R. Role of ultrasound in dengue fever. Br J Radiol 2005; 78: 416-8.
2. Guzman MG, Halstead SB, Artsob H, Buchy P, Farrar J, Gubler DJ, et al. Dengue: a continuing global threat. Nat Rev Microbiol 2010; 8(12 Suppl): S7-16.
3. WHO. Dengue and severe dengue. [online] 2015 May last update [cited 2015 May 16]. Available from: http://www.URL: www.who.int/mediacentre/factsheets/fs117/en.
4. Khan E, Hasan R. Dengue Infection in Asia; A Regional Concern. J Postgrad Med Inst 2011; 26: 01-06.
5. Shepherd SM. Dengue. Emedicine [online] 2013 [cited 2015 May 16]. Available from: URL: http://emedicine.medscape.com/article/215480-overview.
6. Khurram M, Qayyum W, Hassan SJ, Mumtaz S, Bushra HT, Umar M. Dengue hemorrhagic fever: Comparison of patients with primary and secondary infections. J Infect Public Health 2014; 7: 489-95.
7. Vaughn DW, Green S, Kalayanarooj S, Innis BL, Nimmannitya S, Suntayakorn S, et al. Dengue viremia titer, antibody response pattern, and virus serotype correlate with disease severity. J Infect Dis 2000; 181: 2-9.
8. World Health Organization. Dengue hemorrhagic fever: diagnosis, treatment, prevention and control. 2nd ed. Geneva, Switzerland: World Health Organization [online] 1997 [cited 2015 May 16]. Available from: URL: http://www.who.int/csr/resources/publications/dengue/Denguepublication/en/.
9. Masud F, Butt TK, Ali M. Dengue Expert Advisory Group (DEAG), Dengue GCP guidelines 2012. Lahore: DEAG; 2012.
10. Comprehensive Guidelines for Prevention and Control of Dengue and Dengue Haemorrhagic Fever. WHO; 2011
11. Centers for disease control and prevention (CDC). Dengue: laboratory guidance and diagnostic testing [online] 2012 September 27 last update [cited 2015 May 16]. Available from: URL: http://www.cdc.gov/dengue/clinicallab/laboratory.html?
12. Gan VC, Lye DC, Thein TL, Dimatatac F, Tan AS, Leo YS. Implications of discordance in world health organization 1997 and 2009 dengue classifications in adult dengue. PLoS One 2013; 8: e60946.
13. Gupta P, Khare V, Tripathi S, Nag VL, Kumar R, Khan MY, et al. Assessment of World Health Organization definition of dengue hemorrhagic fever in North India. J Infect Dev Ctries 2010; 4: 150-5.
14. Sachar S Goyal S, Sachar S. Role of ultrasonography ("honeycomb sign") in early detection of dengue hemorrhagic fever. Arch Clin Exp Surg 2013; 2: 38-42
15. Colbert JA. Assessing the Role of ultrasound to determine prognosis and disease severity in pediatric dengue patients [online] 2008 [cited 2015 May 16]. Available from: URL: http://www.med.stanford.edu/oih/documents/Colbert-TravelScholarProposal.doc
16. Fatima S, Abeddin A, Firdous F. To assess the severity of dengue fever in patients attending a tertiary care teaching hospital using WHO grading system. Der Pharmacia Lettre 2013; 5: 76-80
17. Finding reasons for dengue fever outbreak in Pindi. The News. December 10, 2013 [online] 2013 [cited 2015 May 16]. Available from: URL: http://www.thenews.com.pk
18. Dengue fever spike almost comes to an end in Rawalpindi. The News. December 01, 2013 [online] 2013 [cited 2015 May 16]. Available from: URL:www.thenews.com.pk
19. Oliveira RVB, Rios LTM, Branco MRFC, Braga Júnior LL, Nascimento JMS, Silva GF, et al. Usefulness of ultrasonography in children with suspected dengue hemorrhagic fever: a literature review. Radiol Bras 2010; 43: 401-7.
20. Pramuljo HS, Harun SR. Ultrasound findings in dengue haemorrhagic fever. Pediatr Radiol 1991; 21: 100-2.
21. Balasubramanian S, Janakiraman L, Kumar SS, Muralinath S, Shivbalan S. A reappraisal of the criteria to diagnose plasma leakage in dengue hemorrhagic fever. Indian Pediatr 2006; 43: 334-9.
22. Michels M, Sumardi U, de Mast Q, Jusuf H, Puspita M, Dewi IM, et al. The predictive diagnostic value of serial daily bedside ultrasonography for severe dengue in Indonesian adults. PLoS Negl Trop Dis 2013; 7: e2277
23. Srikiatkhachorn A, Krautrachue A, Ratanaprakarn W, Wongtapradit L, Nithipanya N, Kalayanarooj S, et al. Natural history of plasma leakage in dengue hemorrhagic fever: a serial ultrasonographic study. Pediatr Infect Dis J 2007; 26: 283-90
24. Thulkar S, Sharma S, Srivastava DN, Sharma SK, Berry M, Pandey RM. Sonographic findings in grade III dengue hemorrhagic fever in adults. J Clin Ultrasound 2000; 28: 34-7.
25. Setiawan MW, Samsi TK, Pool TN, Sugianto D, Wulur H. Gallbladder wall thickening in dengue hemorrhagic fever: an ultrasonographic study. J Clin Ultrasound 1995; 23: 357-62.
26. Laoprasopwattana K, Libraty DH, Endy TP, Nisalak A, Chunsuttiwat S, Vaughn DW, et al. Dengue virus (DV) enhancing antibody activity in preillness plasma does not predict subsequent disease severity or viremia in secondary DV infection. J Infect Dis 2005; 192: 510-9.
27. Yousaf KR, Atiq S, Sheikh QS, Nisar MS, Mansoor Z, Khalid S. Sonographic features of polyserositis as an adjunct to clinico-pathological parameters in diagnosing and predicting the severity of dengue fever. Pak J Med Health Sci 2011; 5: 184-9.
28. Richard W. Pleural Diseases. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2007; pp 241
29. Ahmed S, Mohammad WW, Hamid F, Akhter A, Afzal RK, Mahmood A. The 2011 dengue haemorrhagic fever outbreak in Lahore- an account of clinical parameters and pattern of haemorrhagic complications. J Coll Physicians Surg Pak 2013; 23: 463-7.
30. Raza FA, Rehman Su, Khalid R, Ahmad J, Ashraf S, Iqbal M, et al. Demographic and Clinico-Epidemiological Features of Dengue Fever in Faisalabad, Pakistan. PLoS ONE 2014; 9: e89868.
31. Wu KL, Changchien CS, Kuo CH, Chiu KW, Lu SN, Kuo CM et al. Early abdominal sonographic findings in patients with dengue fever. J Clin Ultrasound 2004; 32: 386-8.
32. Sam SS, Omar SF, Teoh BT, Abd-Jamil J, AbuBakar S. Review of Dengue hemorrhagic fever fatal cases seen among adults: a retrospective study. PLoS Negl Trop Dis 2013; 7: e2194.
33. Mia MW, Nurullah AM, Hossain A, Haque MM. Clinical and Sonographic Evaluation of Dengue Fever in Bangladesh: A Study of 100 Cases. Dinajpur Med Col J 2010; 3: 29-34.
34. Ahmed S, Ali N, Ashraf S, Ilyas M, Tariq WU, Chotani RA. Dengue fever outbreak: a clinical management experience. J Coll Physicians Surg Pak 2008; 18: 8-12.
35. Divisional Dengue Expert Advisory Group, Rawalpindi. Report 2013/2014, Rawalpindi: DDEAG, 2014.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: