
Fatima Shahid ( Medical graduate, MBBS, Agha Khan University, Karachi. )
Maria Tariq Siddiqui ( Liaquat National Hospital and Medical College, University of Karachi. )
Muhammad Muneer Amanullah ( Congenital Cardiothoracic Surgery, Department of Surgery, Aga Khan University, Karachi. )
May 2015, Volume 65, Issue 5
Original Article
Abstract
Objective: To evaluate patients presenting with Tetralogy of Fallot with absent pulmonary valve syndrome to a tertiary care hospital and their surgical management.
Methods: The retrospective study was conducted at Congenital Cardiac Services, Aga Khan University Hospital, Karachi, Pakistan, and comprised data of Tetralogy of Fallot patients between April 2007 and June 2012. Data was analysed together with follow-up echocardiography. Variables assessed included demographics, imaging, operative technique, complications, post-operative recovery and follow-up echocardiography. SPSS 17 was used for statistical analysis.
Results: Of the 204 patients, 6 (3%) had undergone surgical correction for Tetralogy of Fallot with absent pulmonary valve syndrome. All 6(100%) patients underwent complete repair. Median age for surgery was 8.5 years (range: 0.5-29 years). Of the different surgical strategies used, Contegra and Bioprosthetic valve placement had satisfactory outcome with minimal gradient at Right Ventricular Outflow Tract, good ventricular function and mild valvular regurgitation. One (16.6%) patient with Trans Annular Patch developed post-operative Right Ventricle Outflow Tract gradient of 80mmHg with moderate pulmonary regurgitation. One (16.6%) patient with monocusp valve developed free pulmonary regurgitation at 6 months. The other 4(66.6%) patients are currently free from any complications or re-intervention.
Conclusion: Early surgery is preferred in symptomatic patients. The repair depends upon achieving integrity of pulmonary circulation which is best achieved by using right ventricle to pulmonary artery conduit or inserting a pulmonary valve.
Keywords: Absent pulmonary valve syndrome, Contegra valved conduit, Pulmonary valve replacement, Trans-annular patch. (JPMA 65: 467; 2015).
Introduction
Absent Pulmonary Valve Syndrome (APVS) is a rare variant and makes up about 3-6% of patients of Tetralogy of Fallot (ToF).1 Apart from the hallmark features of ToF, these patients have an absent/rudimentary pulmonary valve, leading to pulmonary regurgitation during foetal life, causing aneurysmal dilatation of pulmonary vessels, compressing the trachea or the main stem bronchi, and leading to tracheomalacia and bronchomalacia. Patients present in early infancy with respiratory symptoms, but some reach adulthood undetected. The debate continues whether to operate early, insert pulmonary valve or operate when respiratory symptoms develop.
The current study was planned to review the management and outcomes of surgical interventions.
Patients and Methods
The retrospective chart review and prospective follow up was conducted at Congenital Cardiac Services, Aga Khan University Hospital, Karachi, Pakistan, and comprised data of patients with ToF and APVS between April 2007 and June 2012. Data was analysed together with follow-up echocardiography. Institutional policy did not require ethical review committee\'s approval for retrospective analyses. Demographics, pre-operative echocardiogram and computed tomography (CT) angiogram findings together with operative data, complications and post-operative echocardiographic analysis were recorded on a pre-designed proforma. Data was analysed using SPSS 17 and was expressed as median and minimum-maximum ranges where appropriate.
All operations had been performed via a median sternotomy. Cardiopulmonary bypass (CPB) was established with aortic and bi-caval cannulation and moderate hypothermia of 28°C. Aortic cross-clamping was applied and myocardial preservation was maintained with intermittent ante-grade cold blood cardioplegia for intra-cardiac repair.
Complete repair was performed in all patients. Enlargement of the Right Ventricular Outflow Tract (RVOT) was done by resecting the hypertrophied muscle bundles through a trans-annular patch and infundibular incision that was made to serve as a site of the Right Ventricle (RV) to Pulmonary Artery(PA) conduit and relief of RVOT obstruction (RVOTO). PA reduction arterioplasty was performed in patients by excising elliptical strips of the anterior PA wall.
The Ventricular Septal Defect (VSD) was closed with a patch of Dacron through a right atriotomy.
Following closure of the VSD, the left heart was de-aired and the aortic cross-clamp was released. The RV to PA reconstruction was performed with an empty beating heart to minimise myocardial ischaemia time.
RV to PA continuity was restored with a Contegra valved conduit, bioprosthetic valve, monocusp or trans-annular patch. The atriotomy was closed during re-warming. A Patent Foramen Ovale (PFO) was always left behind to vent the RV and prevent RV dysfunction.
Post-operative echocardiography was performed in all patients at the time of discharge, measuring trans-pulmonary pressure gradients and RV ejection fraction (EF).
Follow-up data was obtained in June 2012, corresponding to a midterm follow-up of 17 months (range: 2.5-50 months). Echocardiography was performed to evaluate their RVOT gradient, valve integrity and RV function.
Results
Of the 204 patients, 6 (3%) had undergone surgical correction for ToF with APVS. All 6(100%) patients underwent complete repair. Median age for surgery was 8.5 years (range: 0.5-29 years) (Table-1).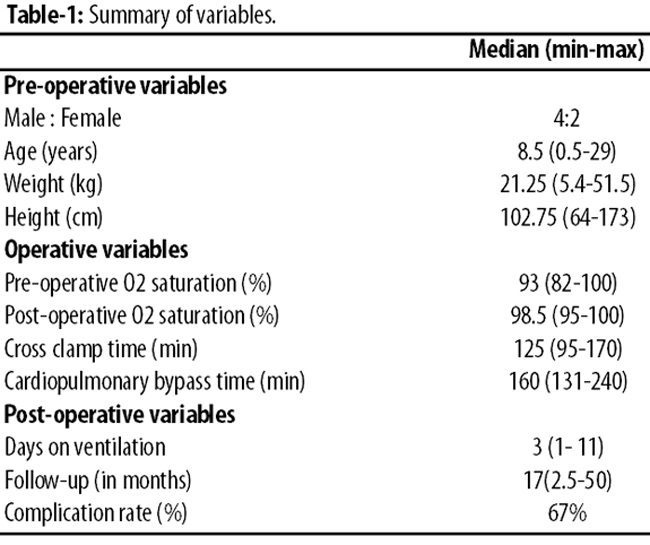
Out of the 6 patients, 5(83.3%) presented with complaints of recurrent respiratory tract infections. The three older patients (age >12 years) had shortness of breath and cough which worsened with exertion or while lying flat. One (16.6%) infant had DiGeorge syndrome.
All patients were undernourished with the median body mass index (BMI) of the older 3(50%) patients being 14.55kg/m2 (range: 11.88-17.52), and the weight and height of the 3(50%) infants were below the fifth percentile.
Pre-operative echocardiograms showed findings consistent with ToF with APVS (Table-2).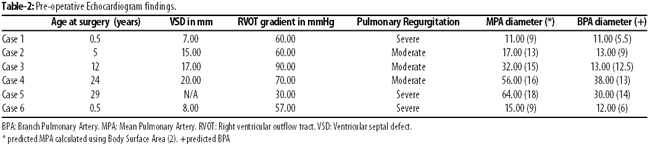
Five (83.3%) patients had large VSD. The remaining patient (No. 5) had his VSD closure during a previous surgery 15 years ago at another hospital. All had severe RVOTO and moderate to severe pulmonary regurgitation. Atrial Septal Defect (ASD) was noted in 1(16.6%) patient (No. 1), and 1(16.6%) had Patent Ductus Arteriosus (PDA) (No.5). All 5 (83.3%) of these patients had significantly large Main Pulmonary Arteries (MPAs) and Branch Pulmonary Arteries (BPAs).
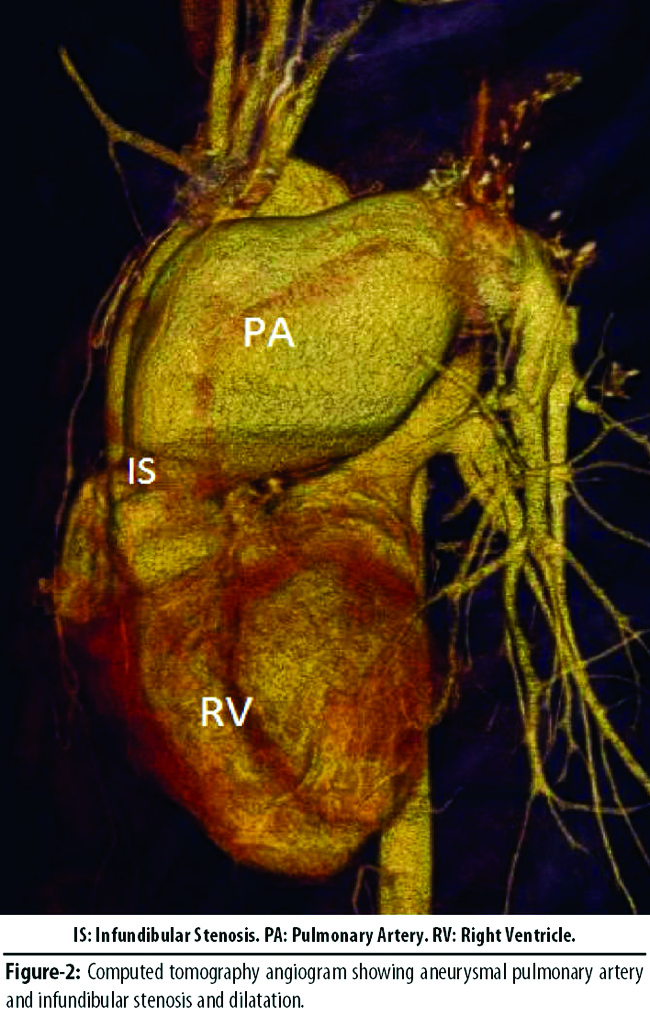
CT angiogram confirmed the findings on echocardiogram. They also showed compression of the trachea and main stem bronchi by the dilated pulmonary arteries (Figures-1 and 2).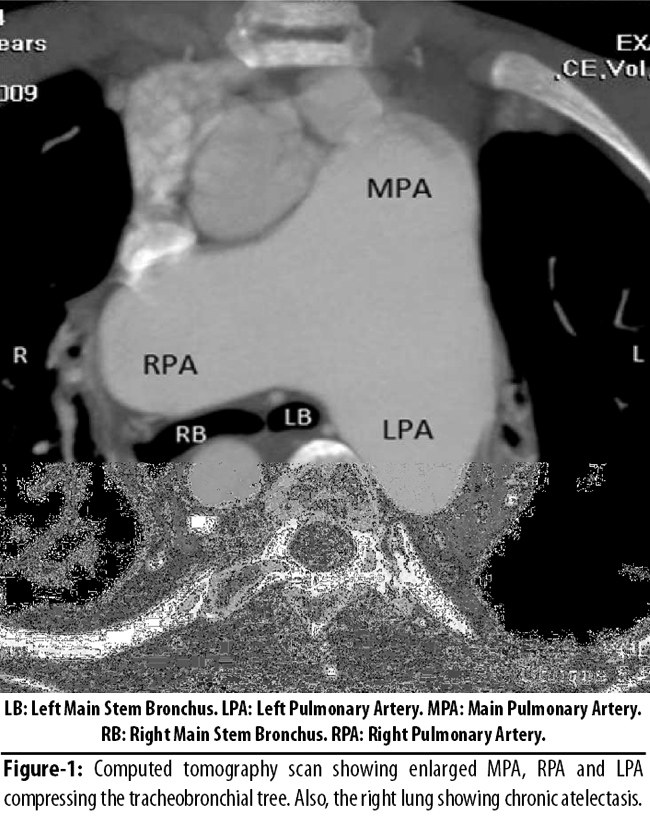
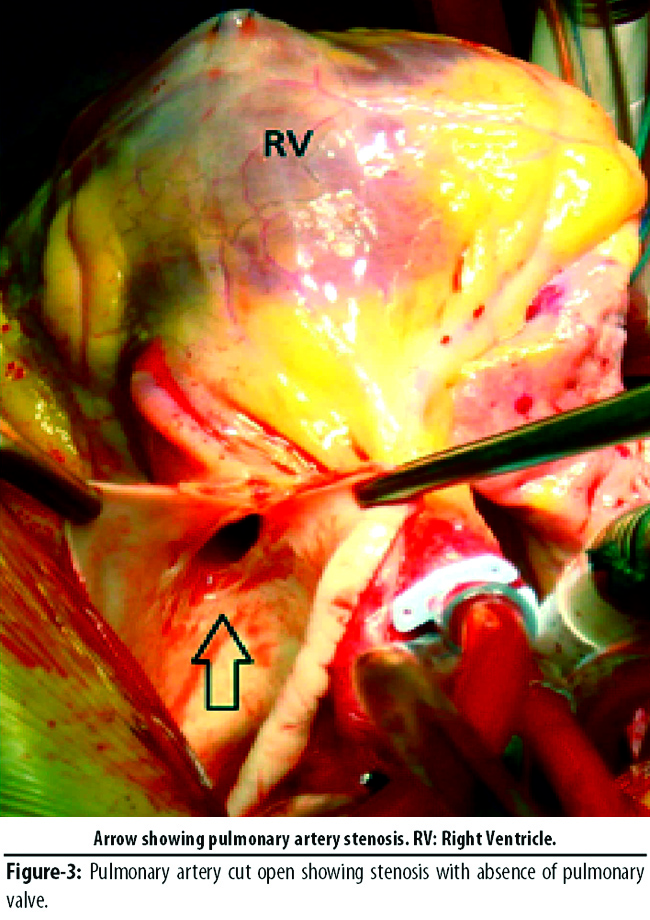
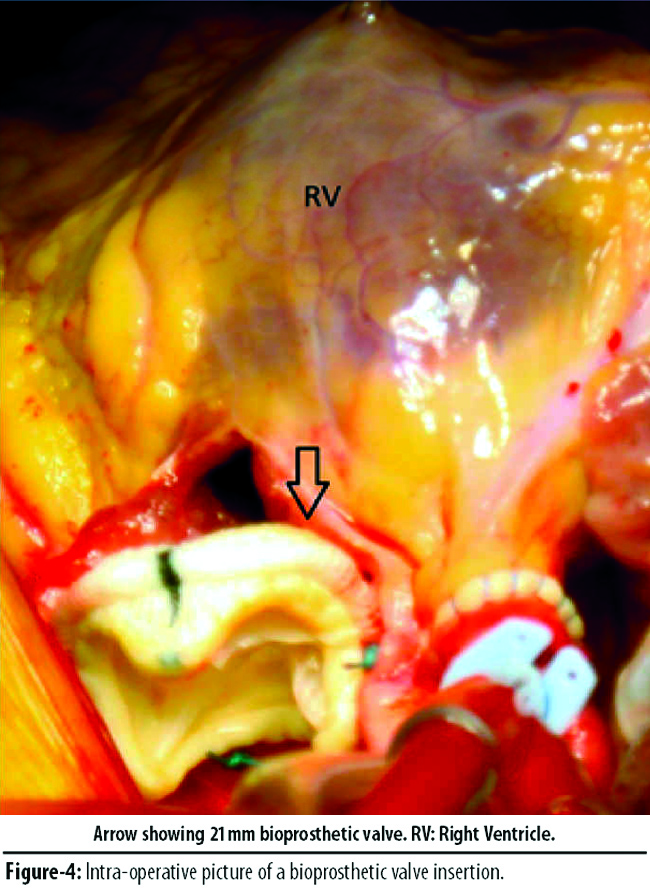
Only 1(16.6%) patient had been previously operated for closure of VSD, while 5(83.3%) were undergoing surgery for the first time. The median by pass time was 160 minutes (range: 131-240 minutes) and cross-clamp time was 125 minutes (range: 95-170 minutes). RV to PA continuity was restored with a Contegra valved conduit in 1(16.6%), bioprosthetic valve in 2(33.3%), monocusp in 2(33.3%) or trans-annular patch (TAP) in 1(16.6%) (Table-3) (Figures-3 and 4).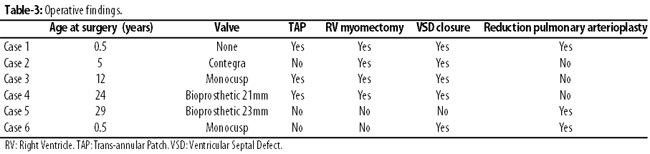
Median time on ventilation was 3 days (range: 1-11 days) and all patients were discharged within a week\'s time after being shifted to the ward (Table-4).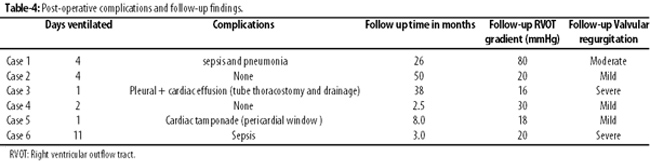
The younger patients were ventilated for longer compared to the older ones. However, the latter group suffered from more post-operative complications i.e. cardiac tamponade and pleural effusion. Case 3 required re-exploration, while Case 5 had the pleural and pericardial collections drained via tube thoracostomy. The reason for the high mediastinal drain output and collection was secondary to post-operative coagulopathy. Since then we have incorporated the use of whole blood and the effect on post-operative bleeding has reduced remarkably.
At follow-up, valve regurgitation was severe in 2(33.3%) patients who had free pulmonary regurgitation. This was secondary to the monocusp valve getting stuck to the under-surface of the TAP. RV function ranged from good to mild dysfunction in the given follow-up time period in all the patients.
Discussion
TOF-APVS is characterised by aneurysmal dilatation of the PAs and atresia or rudimentary development of the pulmonary valve with a hypoplastic annulus. Airway morbidity is what differentiates APVS from other variations of the Fallot\'s anatomical spectrum.2 Tracheobronchial compression by dilated PAs in neonates and infants is the cause of respiratory symptoms.3 Approximately half of ToF with APVS patients present in infancy with respiratory symptoms.4
Patients of ToF with APVS can be sub-divided into two distinct groups depending on age and symptoms; those who present with respiratory symptoms in early infancy, and those who do not. The latter group is clinically comparable to standard ToF patients.1,4 In our series, despite two distinct age groups, all patients showed respiratory symptoms rather than ToF symptoms. The older group (>12 years), had milder symptoms compared to the younger patients.
Although there is no concrete consensus on the timing of surgery, early primary repair should always be considered. In infants with life-threatening airway obstruction surgery is necessitated due to poor prognosis with medical treatment.5 However, the two main questions regarding repair are whether a prosthetic pulmonary valve should be inserted and secondly whether to perform pulmonary reduction arterioplasty along with the classical ToF repair.
Insertion of pulmonary valve remains a controversial subject. In one study, monocusp valve did not prevent significant pulmonary incompetence at late follow-up. Moreover, complications such as calcification and stenosis of the prosthetic valve may require future reoperations for pulmonary valve replacement.5 For this reason some authors suggest delaying surgery in older asymptomatic children.6
The presence and severity of respiratory distress are the deciding factors in pulmonary reduction arterioplasty. In patients with respiratory compromise, a pulmonary reduction arterioplasty is performed which may be combined with a Le\'compte manoeuvre.4 Sometimes despite repair of primary lesion, these patients continue to have a complicated course because of irreversible changes in the airways (bronchomalacia or tracheomalacia) secondary to prolonged extrinsic vascular compression during peri-natal development.4,5,7
As dictated by their respiratory symptoms, three of the six patients underwent pulmonary reduction arterioplasty. Out of these, the two younger patients had no valve inserted, while the older one had a bioprsothetic valve (Case 5) and showed satisfactory post-operative results. A prosthetic valve was not inserted in the younger patients as it would have been too large for the small pulmonary arteries, which may have led to compression of left circumflex artery running posteriorly and compromising the blood supply to the myocardium.
In the remaining three patients a classic ToF repair was done. Case 3 had ToF repair with a monocusp, and this patient developed free pulmonary regurgitation two years after surgery. The other two valves used were the Contegra (valved conduit) and the bioprosthetic valve. Younger age at operation is associated with improved late survival although most children will require RVOT re-operation after outgrowing the conduit.8 There is also a significant incidence of conduit-related complications, particularly with the smaller conduits.9 In our case, Contegra showed a favourable outcome in the five-year follow-up time with only mild regurgitation and gradient of 15mmHg.
On follow-up, majority of the patients remained free of long-term complications and re-intervention.
The high RVOT gradient of 80mmHg (Case 1) was an unexpected outcome, but pulmonary stenosis may have developed because of incomplete infundibular resection trying to prevent free pulmonary regurgitation in the post-operative period. The parents were counselled about the need of re-operation in order to relieve the high RVOT gradient, but the patient was unfortunately lost to follow-up, a situation not unheard of in a third world country.
There is little data regarding the long-term prognosis after repair of ToF with APVS. We believe that the current clinical strategy dictating the use of a pulmonary reduction arterioplasty in patients with respiratory compromise, restoration of pulmonary valve competence along with post-operative ventilator management results in an effective outcome. Due to the small number in our series, however, we cannot comment about long-term consequences.
Conclusion
ToF with APVS is a rare syndrome. Historically, early surgery has been preferred, but the hallmark of repair depends upon relieving airway compression, establishing valve competency and achieving integrity of the pulmonary circulation. Infants may require a more aggressive post-operative ventilatory support and future RVOT reoperations compared to older children.
References
1. Kirshbom PM, Kogon BE. Tetralogy of Fallot with absent pulmonary valve syndrome. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu 2004; 7: 65-71.
2. Norgaard MA, Alphonso N, Newcomb AE, Brizard CP, Cochrane AD. Absent pulmonary valve syndrome. Surgical and clinical outcome with long-term follow-up. Eur J Cardiothorac Surg 2006; 29: 682-7.
3. Kreutzer C, Schlichter A, Kreutzer G. Tetralogy of Fallot with absent pulmonary valve: a surgical technique for complete repair. J Thorac Cardiovasc Surg 1999; 117: 192-4.
4. Hraska V, Photiadis J, Schindler E, Sinzobahamvya N, Fink C, Haun C, et al. A novel approach to the repair of tetralogy of Fallot with absent pulmonary valve and the reduction of airway compression by the pulmonary artery. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu 2009:59-62.
5. Godart F, Houyel L, Lacour-Gayet F, Serraf A, Sousa-Uva M, Bruniaux J, et al. Absent pulmonary valve syndrome: surgical treatment and considerations. Ann Thorac Surg 1996; 62: 136-42.
6. Chavez IM, Solano JF, Quispe JA, de Micheli A, Hernandez AB, Marroquin SR. Absent pulmonary valve syndrome. Evaluation, surgical treatment and risk factors. Arch Cardiol Mex 2008; 78: 79-86.
7. Conte S, Serraf A, Godart F, Lacour-Gayet F, Petit J, Bruniaux J, et al. Technique to repair tetralogy of Fallot with absent pulmonary valve. Ann Thorac Surg 1997; 63: 1489-91.
8. Bove T, Demanet H, Wauthy P, Goldstein JP, Dessy H, Viart P, et al. Early results of valved bovine jugular vein conduit versus bicuspid homograft for right ventricular outflow tract reconstruction. Ann Thorac Surg 2002; 74: 536-41
9. Shebani SO, McGuirk S, Baghai M, Stickley J, De Giovanni JV, Bu\'lock FA, et al. Right ventricular outflow tract reconstruction using Contegra valved conduit: natural history and conduit performance under pressure. Eur J Cardiothorac Surg 2006; 29: 397-405.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: