
Yashdeep Gupta ( Department of Endocrinology, Government Medical College and Hospital, Chandigarh, India. )
Bharti Kalra ( Department of Obstetrics and Gynaecology, Bharti Hospital, Karnal, India. )
May 2015, Volume 65, Issue 5
Editorial
The prevalence of diabetes in adults in Middle-East and North Africa Region is 9.2%, of which half are undiagnosed, and at considerable risk of complications.1 Though ideally, universal screening should be carried out to detect these cases, we may need to target high risk groups to maximize benefits. Women with gestational diabetes mellitus (GDM) form a high risk cohort which can be targeted for primary prevention of diabetes.
While the importance of antenatal screening for GDM is well recognised, postpartum follow up is often ignored. Health care providers, and women in their care, find it challenging to understand and implement the various components of post partum GDM care. We propose a patient- and physician-friendly mnemonic, the ABCDEFG (Table-1)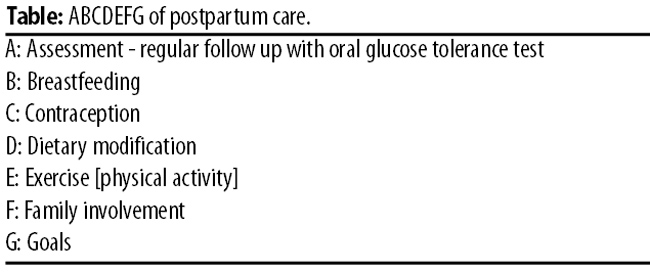
of postpartum care, which can serve public media and policy makers as well.
A: Assessment
Timely identification of prediabetes/diabetes, to prevent complications, is the primary aim of screening. Hence, \'A\' stands for assessment. American Diabetes Association recommends 75 gram oral glucose tolerance test (OGTT) 6 weeks after delivery, with repeat screening at 3 years, if values are normal, and yearly, if prediabetes is detected.2 As 5-year diabetes conversion rates are nearly 50%,3 frequent screening is warranted in South Asians. Annual screening in women with normal glucose tolerance, and 3-6 monthly testing in women identified to have prediabetes, for at least 10 years post-delivery, is prudent in women with risk factors like diagnosis in early pregnancy, obesity, history of insulin use, and high-risk ethnicity. Barriers to postpartum screening should be assessed, and appropriate measures taken to ensure universal screening.
B: Breastfeeding
Postpartum management is not glucocentric, and nursing should never be forgotten. The \'B\' in our mnemonic represents breastfeeding, which reduces development of diabetes in women. Lactating women have 60% lower odds of persistent dysglycaemia than non-lactating mothers.4 Higher lactation intensity at 6-9 weeks postpartum is inversely associated with fasting plasma glucose and insulin concentrations.5 Lactation is characterized by increased glucose utilization and lipolysis for milk production, as well as by higher maternal basal metabolic rates and mobilization of fat stores. Breastfeeding should be encouraged in women with GDM.
C: Contraception
\'C\' [contraception], an integral part of the "follow up formula", helps delay pregnancy and reduces further metabolic risk. An additional pregnancy increases the risk of development of diabetes by 3.34 times, compared with women without an additional pregnancy, after GDM in index pregnancy.6 Unplanned pregnancies, conceived when gluco-metabolic risk factors are inadequately controlled, are associated with increased feto-maternal risks. Therefore, effective contraception is essential.
History of GDM does not impact choice of contraceptive method. Low dose combined oral contraceptives are safe and effective.7 Intrauterine devices, barrier methods and tubal ligation do not impact diabetes risk.8 Progestin-only preparations have been associated with increased diabetes risk in observational studies, but a cause-and-effect relationship has not been established.8 Therefore, person-centric decision-making should inform the choice of contraception in women with GDM.
D. Diet
Postpartum follow up includes not only screening, but encompasses healthy lifestyle counselling. This is our \'D\' [diet] and \'E\' [exercise]. Healthier diets are associated with decreased risk of diabetes. Nurses with history of GDM who were adherent to, or were in the highest quartile of the Mediterranean diet scale, had 40% lower risk of diabetes compared with women in the lowest quartile.9 Hence, a culturally appropriate, individualized, diet plan should be made for each woman, considering her lactational demands as well.
E. Exercise
Intensive lifestyle change, targeting 7% reduction in weight, and increased physical activity, is able to achieve 53% reduction in diabetes incidence.10 The incidence of diabetes in women with GDM randomized to lifestyle was 7.4/100 person-years, compared with 15.2 in the placebo group, in the Diabetes Prevention Programme.
The feasibility or adoption of lifestyle modification may be limited among recently delivered women, as they have to meet nursing and parenting demands. Therefore, our mnemonic includes \'F\' [family] along with DE.
F: FAMILY
The family is an important determinant of health in Afro-Asia. Family-oriented motivation and education, regarding lifestyle modification, targeting the mother-in-law and female household members, is necessary. With knowledge, women can improve the family\'s lifestyle and health, including that of their children. They can motivate neighbours and community members as well. The family should also be encouraged to help women with GDM adhere to healthy lifestyle and follow up regularly.
G: Goals
The success of any activity is measured against pre-set goals. This is the \'G\' of our mnemonic. Women with GDM are more likely to experience cardiovascular events, at earlier ages than their euglycemic peers.11 Women with histories of GDM have elevated blood pressure and unfavourable lipid profiles.12 The characteristics of metabolic syndrome, may appear at 3 months postpartum. This implies the need to monitor cardiometabolic parameters regularly.
Blood pressure should be assessed at each visit. Lipids should be assessed at baseline, and after 2 to 5 years in low-risk women.12 Weight control is important, as overweight/obese women who lose weight (2.0 kg/m2) after their index pregnancy lower their risk of future GDM by almost 80%.13 Goals of ideal body weight, glucose, blood pressure, and lipid levels should be shared with the woman and her family, and every effort made to achieve the same.
Conclusion
The importance of postpartum follow up of women with GDM cannot be underestimated. This life-stage provides an opportunity for regular screening for metabolic risk factors, periodic assessment of goals, and reinforcement of nursing, contraceptive and lifestyle advice.
The ABCDEFG model helps simplify postpartum management of GDM, encourages regular follow up, healthy lifestyle and child bearing practices, and facilitates achievement of optimal cardiometabolic goals.
Its simplicity allows its use as a pedagogic tool, a reminder on maternity cards/consultation slips, a social marketing strategy for public media, and a buzzword for policy makers. We hope that postpartum management of GDM will become as simple as ABCDEFG.
References
1. Majeed A, El-Sayed AA, Khoja T, Alshamsan R, Millett C, Rawaf S. Diabetes in the Middle-East and North Africa: an update. Diabetes Res Clin Pract 2014; 103: 218-22.
2. American Diabetes Association. Standards of medical care in diabetes-2014. Diabetes Care 2014; 36 (suppl 1): S14-80.
3. Kale SD, Yajnik CS, Kulkarni SR, Meenakumari K, Joglekar AA, Khorsand N, et al. High risk of diabetes and metabolic syndrome in Indian women with gestational diabetes mellitus. Diabet Med 2004; 21: 1257-8.
4. O\'Reilly MW, Avalos G, Dennedy MC, O\'Sullivan EP, Dunne F. Atlantic DIP: high prevalence of abnormal glucose tolerance post partum is reduced by breastfeeding in women with prior gestational diabetes mellitus. Eur J Endocrinol 2011; 165: 953-9.
5. Gunderson EP, Hedderson MM, Chiang V, Crites Y, Walton D, Azevedo RA, et al. Lactation intensity and postpartum maternal glucose tolerance and insulin resistance in women with recent GDM: the SWIFT cohort. Diabetes Care 2012; 35: 50-6.
6. Peters RK, Kjos SL, Xiang A, Buchanan TA. Long-term diabetogenic effect of single pregnancy in women with previous gestational diabetes mellitus. Lancet 1996; 347: 227-30.
7. Gourdy P. Diabetes and oral contraception. Best Pract Res Clin Endocrinol Metab 2013; 27: 67-76.
8. Buchanan TA, Page KA. Approach to the patient with gestational diabetes after delivery. J Clin Endocrinol Metab 2011; 96: 3592-8.
9. Tobias D, Hu F, Chavarro J, Rosner B, Mozaffarian D, Zhang C. Healthful dietary patterns and type 2 diabetes mellitus risk among women with a history of gestational diabetes mellitus. Arch Intern Med 2012; 172: 1566-72.
10. Ratner R, Christophi C, Metzger B, Dabelea D, Bennett P, Pi-Sunyer X, et al. Prevention of diabetes in women with a history of gestational diabetes; effects of metformin and lifestyle interventions. J Clin Endocrinol Metab 2008; 93: 4774-9.
11. Shah BR, Retnakaran R, Booth GL. Increased risk of cardiovascular disease in young women following gestational diabetes mellitus. Diabetes Care 2008; 31: 1668-9.
12. Mielke RT, Kaiser D, Centuolo R. Interconception care for women with prior gestational diabetes mellitus. J Midwifery Womens Health 2013; 58: 303-12.
13. Ehrlich S, Hedderson M, Feng J, Davenport E, Gunderson E, Ferrara A. Change in body mass index between pregnancies and the risk of gestational diabetes in a second pregnancy. Obstet Gynecol 2011; 117: 1323-30.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: