
Muhammad Akram ( Postgraduate Medical Institute, Lahore. )
Muhammad Shoaib Akhtar ( Postgraduate Medical Institute, Lahore. )
Nusrat Waqar ( Department of Physiology and Pharmacology, University of Agriculture, Faisalabad. )
November 1982, Volume 32, Issue 11
Original Article
Abstract
Glomerular Filtration Rate (GFR) was determined in non-pregnant, fullterm pregnant (38-40 weeks of gestation) and post-puerperal (8-12 weeks post-partum) women. GFR. was determined by 24 hours-endogenous creatinine clearance method. In addition, serum and urinary proteins were estimated in these women to examine whether or not these parameters were also associated with the possible alterations of GFR during pregnancy.
The data obtained revealed that GFR is considerably higher in Pakistani women as compared to the values reported from temperate countries. At full term, GFR was observed to fall significantly. The mechanism of fall might be some hormonal influ-ence working in terminal stages of pregnancy. The GFR returns to normal after 8-12 weeks of puerperium. Total serum proteins at terminal stage of pregaancy were significantly lower than non-pregnant levels. During post-puerperal stage, they were slightly raised but there was no significant difference from the levels in the full term pregnancy. In pregnancy total excretion of urinary protein increased significantly than in the nonpregnant women, indicating a functional proteinuria. The total urinary protein levels apparently returned to normal after puerperium as the values were not significantly different from non-pregnant stage. This may be due to removal of the physiological stresses of pregnancy. Low GFR during terminal pregnancy was found to be associated with proteinuria (JPMA 32.257, 1982).
Introduction
Glomerular filtration rate (GFR) is a central feature of renal function and is the basis of most clinical tests and has been suggested to be employed as an aid in the management of pregnancies complicated with hypertension and acute toxaemia (Karim et al., 1976). Considerable literature indicates much disagreement on the extent and patterns of GFR changes especially during pregnancy. Some workers have reported an increase in GFR in early pregnancy which falls towards the normal non-pregnant level at term (Bucht, 1951; Sohar et al, 1956; Buttcrmann, 1958; Gylling, 1961). However, GFR has been observed to be raised persistently throughout pregnancy by Brandstetter and Schuller (1956), Sims and Krantz (1958) and Dignam et al. (1958). On the contrary, it has been demonstrated to fall significantly in late pregnancy (Chesley and Sloan, 1964; Davison and Hytten, 1974). Moreover, majority of these studies, have been carried out in temperate climate and there is little corresponding information about GFR changes during pregnancy in the tropics. Therefore, in an effort to preliminarily estimate the normal GFR values in local women and to study its changes during and after pregnancy, its values were determined in normal (non-pregnant), pregnant (38-40 weeks) and post-puerperal (6-12 weeks post-partum) Pakistani women. In addition, it was also considered imperative to study the changes in blood and urine protein levels because their changes might also be associated with the alterations of GFR during terminal stage of pregnancy.
Material and Methods
Chemicals Used
The chemicals and reagents used were extra-pure and of the analytical grade. They were obtained from E. Merck, Damstadt, West Germany and B.D.H. Laboratories, Poole, England. The protein standard (LabtrolR) used was that of Dade Diagnostics, Miami, U.S.A.
Determination of GFR by Endogenous Creatinine Clearance
Creatinine was estimated in serum and urine by alkaline picrate method (Jaffe\'s Reaction) as described by Bonsnes and Taussky (1945). The urinary levels of creatinine were higher than its serum concentration. Therefore, the urine samples were first diluted to 1:100 with the distilled water. The optical densities were recorded by using Carl Zeiss Spectrophotometer Model PM4 against the blanks. The 24 hour endogenous creatinine clearance (ECC) was calculated by the following formula:
UcxV
ECC ----------
Pc
Uc = Concentration of Creatinine in Urine (mg/100 ml),
Pc = Concentration of Creatinine in Serum (mg/100 ml), and V = is Volume of Urine excreted per minute (ml/min).
Determination of Total Serum and Urine Proteins
The method of Kingsley (1939) was applied for the estimation of total serum proteins using the biuret reaction. The samples and standards were read against the biuret blank at 555 n.m. by using Carl-Zeiss Spectrophotometer. The serum blank was prepared from the opalescent or highly pigmented sera. Turbidimetric method of Henry et al. (1956) was followed for the determination of total urinary proteins. The turbidity was read against the blank at 420 n.m. by using Spectrophotometer.
Statistical Analysis
The values are given as Means±Standard Error of Means (S.E.M.) and Student "t" test was applied to check their significance.
Results
Mean age of 30 normal apparently healthy non-pregnant women was 28.5±1.2 years while 29 pregnant women at terminal stage of pregnancy had a mean age of 29.7±0.9 years. Twenty post-puerperal women were at the age of 29.2 ±0.9 years. Statistically, no significant difference was present between the three groups. In addition, the surface areas calculated from body weights and heights of these subjects were also not significantly different in all groups. The urine volumes in normal, pregnant and post-puerperal women were 1080±57.6, 849 6 ±43.2 and 993.6±57.6 ml/24 hours, respectively. The total urinary volume was significantly less in terminal pregnant women than in non-pregnant women. The urine flow rate was 0.75±0.04, 0.59±0 03 and 0.69±0 04 ml/min in normal, terminal pregnant and post-puerperal cases, respectively.
GFR Determined by Endogenous Creatinine Clearance (ECC)
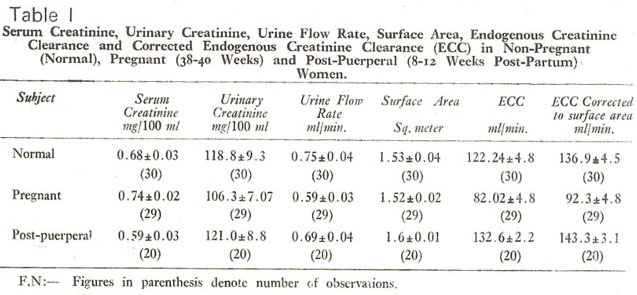
Table I shows the serum and urinary levels of creatinine, urine flow rates, surface areas and the calculated ECC values. The corrected ECC values to the standard body surface area of 1.73 square meter were 136.9±4.5 ml/min, 92.3±4.8 ml/min and 143.3 ± .1 ml/min in normal, terminal pregnant and post-puerperal women respectively (Table I). The GFR thus estimated by calculating the ECC was found to be significantly decreased (P <0.001) in the pregnant women. The GFR in post-puerperal women was significantly higher (P<0.01) than in pregnant group but not significantly different (P>0.05) from the normal non-pregnant women (Table II).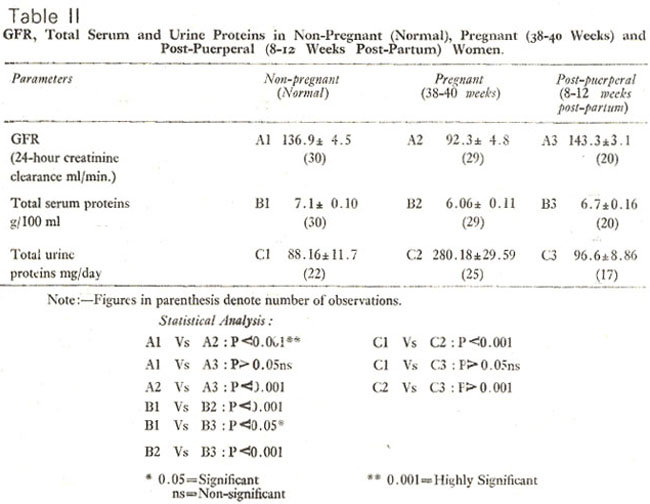
Total Serum and Urine Proteins
The total serum proteins were found to be 7.1±0.10 g/100 ml, 6.06±0 11 g/100 ml and 6 7±0.16 g/10 ml in non-pregnant, terminal pregnant and post-puerperal women respectively (Table II). Serum proteins were significantly less (P <0 001) in pregnant group than in normal, and significantly less in pregnant (P<0.001) group as compared with the post-puerperal groups (Table II). The total urinary proteins in non-pregnant women were 88.16±11.7 mg/day, while the pregnant group had 280.18±29 59 mg/day. Total urinary protein level in post-puerperal women was 96.6±8\' 86 mg/day. The urinary proteins were . ignificantly more in pregnant group (P<0 001) than in both normal and post-puerperal groups (P<10.001).
Discussion
Assessment of glomerular filtration rate (GFR) in human beings is usually carried out by determining the plasma clearance of substances which are freely filterable at glomerulus, neither reabsorbed nor secreted at the tubular level and are not metabolized in the body. One of the methods of choice for the assessment of GFR especially during pregnancy is the determination of endogenous creatinine clearance (Brochner-Mortensen and Rodbro, 1976). This method has been observed to be the most sensitive clinical indicator of early renal disease and gives values usually not too different from the clearance of insulin (Davison and Hytten, 1974; Crowe and Hatch, 1977). Moreover, 24 hours-endogenous creatinine clearance has been reported to reduce the effect of inaccurate timing and faulty bladder emptying (Sirota et al., 1950). It was due to these reasons that this method was selected for the present studies.
GFR Determined By Endogenous Creatinine Clearance (ECC)
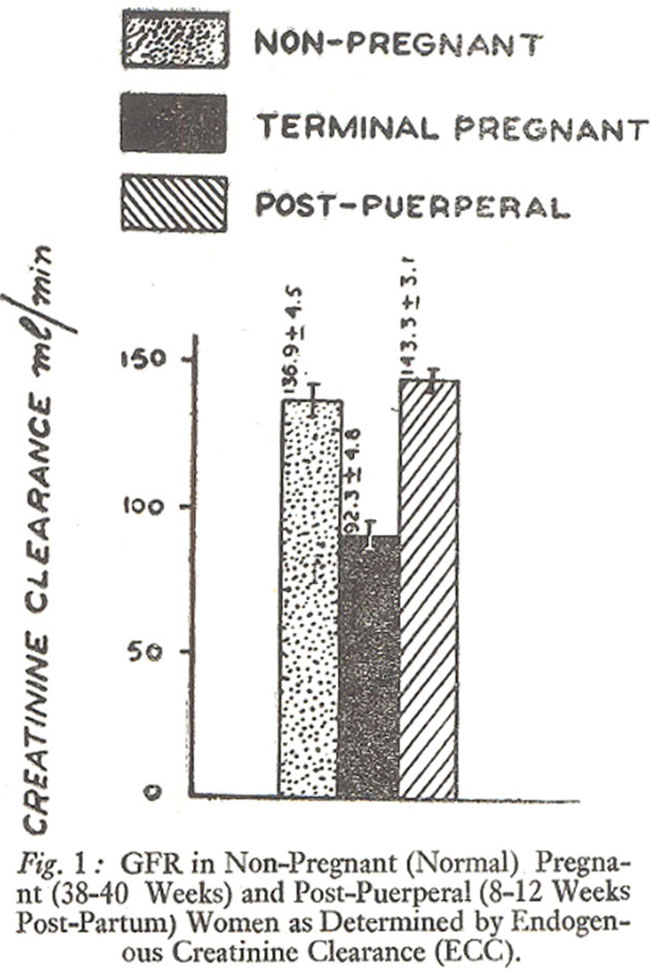
Figure 1 shows that the 24 hours-ECC in normal non-pregnant Pakistani women was 136.9±4.5 ml/min in the present study. This appears to be higher than those observed in other studies including Doolan et al. (1962) who have reported the 24-hours ECC value of 97.7±9.6 ml/min. Similarly, Tobias et al. (1962) observed that 24-hour ECC in nonpregnant women was 95 4±18 ml/min. Edwards and Whyte (1959) have reported the 24-hour ECC as 103 8±13 8 ml/min. The data seem to indicate that GFR in local nonpregnant women is substantially higher than that reported mostly from temperate countries. This may be due to the differences in the dietary habits, socio-economic status and temperate climate of this country. Recently, Athar et al. (1981) have also reported higher GFR in 65 normal male and female Pakistanis.
At terminal stage of pregnancy (38-40 weeks) GFR was. found to be 92.3±4.8 ml/min in our series (Figure 1). This value is about 40 per cent lower than the nonpregnant stage. This observation is in accordance with the findings of Chesley and Sloan (1964) and Davison and Hytten (1974) who have also observed a fall in GFR in late pregnancy. The mechanism responsible for the fall of 24-hour ECC at terminal pregnant stage was not investigated in this study; however, it may be inferred from others that it may be due to some disturbance of glomerulo-tubular balance (Davison and Hytten, 1974). Smith (1951) has reported that pain and fright which are commonly observed at term of pregnancy can also reduce the GFR. Another cause of fall as suggested by Chesley and Sloan (1964) may be the supine posture but Dunlop (1976) has demonstrated that no significant differences in GFR during adoption of various postures (supine, silting and standing). Therefore, some other undefined hormonal or biochemical influences may be responsible for a decrease in GFR at terminal stage of pregnancy.
Total Serum Proteins and GFR
Table II shows that the total serum proteins in non-pregnant women were found to be 7.11 ±0.1 g/100 ml in the present study. Similar level of total proteins in serum has also been reported by several other workers. For example, Alvarez et al. (1959), MacGillivary and Tovey (1957) and Robertson (1969) have reported values of 7.18 g/100 ml, 7.1 g/100 ml, and 7.04 g/100 ml, respectively. At terminal stage of pregnancy (38-40 weeks), total serum proteins were decreased to 6-06±0.11 g/100 ml (Figure 2)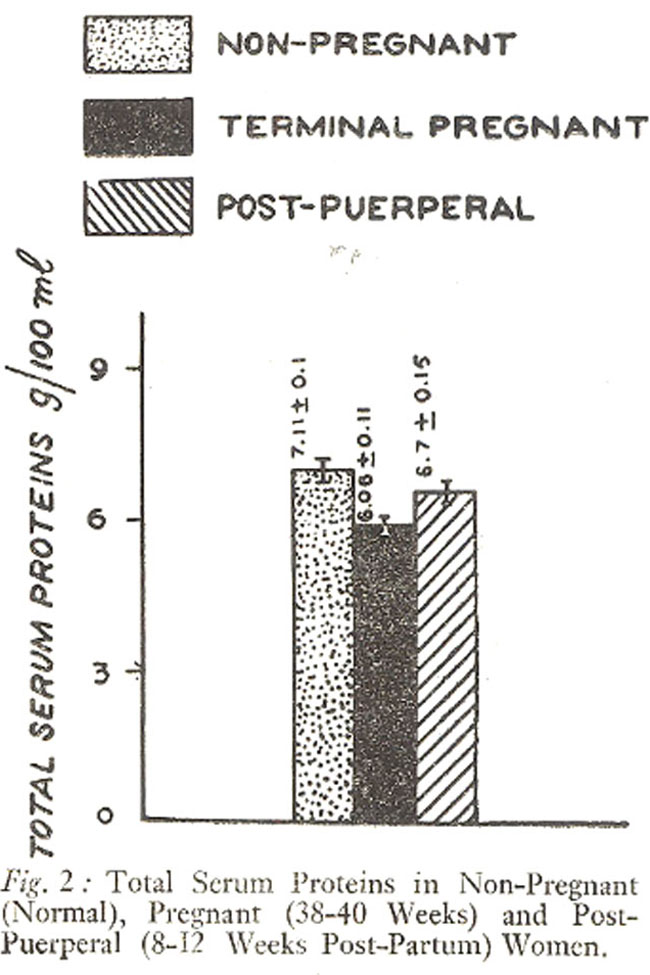
which is also in agreement with the findings of other workers (Alvarez, 1961; Robertson, 1969). The data is in conformity with the well established observation that total serum proteins fall in late pregnancy, mostly due to a relatively large decline of serum albumin (Hytten and Leitch, 1971). The level of total serum proteins in post-puerperal stage (8-12 weeks post-partum) was found to be 6.7 ±0.16 g/100 ml (Table II). This value though significantly lower than the non-pregnant level (P<0.05) but has significantly risen from the terminal pregnant stage. This may be due to dietary habits and socioeconomic status of women in this country. It is clear from the figure 2 that the total serum protein level followed the pattern of GFR alterations during non-pregnant, terminal pregnant, and post-puerperal stages.
Total Urine Proteins And GFR
The total urinary proteins in non-pregnant women were found to be 88.16±11.7 mg/day (Table II). This level is within the range reported by Brobeck (1979), who found that 40-150 mg of proteins are normally excreted per day.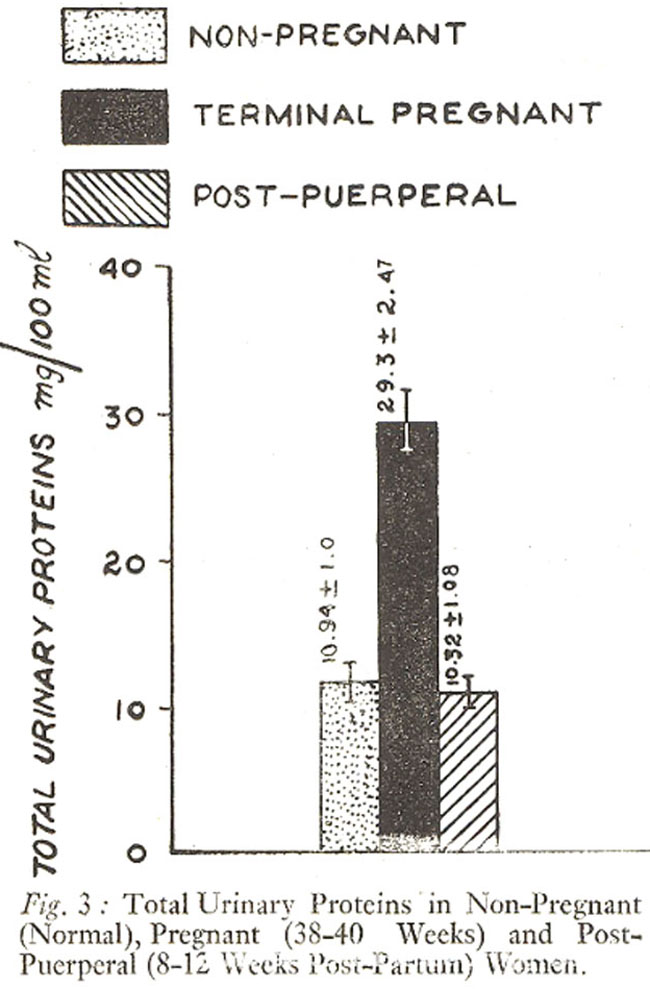
Figure 3 shows that in terminal pregnancy (38-40 weeks), total urine proteins in 24 hours were found to be 280.18 ±29.59 mg/day which is significantly higher (P<0.001) than that of non-pregnant women. This clearly indicates that proteinuria was present during terminal stage of pregnancy. This is in conformity with Berliner and Giebisch (1979), who suggested that proteinuria of about less than 1 g/day may be attributed as functional proteinuria due to physiological stresses. Another mechanism of proteinuria of pregnancy may be, the lordotic posture during this stage of pregnancy (Berliner and Giebisch, 1979). Thus, in contrast to the serum protein levels, the urinary proteins did not follow the pattern of GFR alterations during pregnancy. Inscead, low GFR was found to be associated with high urinary proteins. Figure 3 shows that the excretion of total urinary proteins apparently returned to normal limits after puerperium (96.6±8.86 mg/day) as it is not significantly different from non-pregnant stage. This finding also supports the speculation that the proteinuria of pregnancy was due to physiological stresses of pregnancy as after their withdrawal urine proteins returned to normal during post-puerperal stage. In addition, it may be conjectured that the decrease in serum proteins at terminal pregnancy was due to their increased excretion in urine. However, the decrease of GFR during terminal pregnancy when urinary proteins were increased, cannot be explained at: present.
Conclusion
In conclusion, our data seems to indicate that GFR in local non-pregnant women was consideraoly higher than the reported values from cold climate countries. It significantly fell down (P<0.001) during terminal stage of pregnancy but returned to about normal nonpregnant level at post-puerperal stage. The fall in GFR may be attributed to some hormonal factor operating during pregnancy or some other cause including the prevention of production of angiotensin-II (Jones and Singer, 1978). The total serum protein level was found to be significantly (P<0.001) reduced in terminal pregnancy which coincided with fall in GFR during terminal pregnancy. At terminal pregnancy a highly significant (P<0.001) proteinuria was observed but the normal level of urinary proteins was again obtained at post-puerperal stage. Whether or nor proteinuria was responsible for the fall of GFR observed in this study, still remains to be established. It is, therefore, suggested that the factors responsible for the fall in GFR at terminal pregnancy should be further investigated. To further establish the normal GFR values in the local population, more elaborate studies should be carried out at various research centres and at various seasons of the year.
Acknowledgements
Authors thank Dr. Mushtaq Ahmed, A.H. Nagi and Farrukh A. Khan for their constructive criticism and useful suggestions. Expert technical assistance of Mr. Fazal Haq is also thankfully acknowledged.
References
1. Alvarez, R.R., Gaiser, D.F., Simkins, D.M., Smith, E.K. and Bratvord, G.E. (1959) Serial studies of serum lipids in normal human pregnancy. Am. J. Obstet. Gynaecol., 77:743.
2. Athar, H.S.A., Sallal, I.J.A. and Hasnain, S.N. (1981) Age adjusted creatinine clearance in normal subjects and in patients with renal disorders. JPMA., 31:225.
3. Berliner, R.W. and Giebisch, G. (1979) Body fluids and excretion of urine, in Best and Taylor\'s physiological basis of Medical practice. Editor John R. Brobeck. Sec. 5. 10th ed. Baltimore, Williams and Wilkins, 1979, pp.1-94.
4. Bonsnes, H.W. and Taussky, H.H. (1945) On colori-metric determination of creatinine by Jaffe reaction. J. Biol. Chem., 158:581.
5. Brandstetter, F. and Schuller, E. (1956) Investigations of renal clearance in pregnancy. Contribution to physiology and pathology of kidney and liver in pregnancy. Fortschr. Geburtsch. Gynak. No. 14.
6. Brobeck, J.R. (1979) Body fluids and excretion of urine. In Physiological Basis of Medical Practice. 10th edition. Sec. 5, pp 1-95. The Williams and Wilkins Co., Baltimore.
7. Brochner-Mortensen, J. and Rodbro, P. (1976) Selection of routine method for determination of glomerular filtration rate in adult patients. Scand. J. Clin. Lab. Invest., 36:35.
8. Bucht, H. (1951) Studies on renal function in man with special reference to glomerular filtration and renal plasma flow in pregnancy. Scand. J. Clin. Lab. Invest., 3 (Suppl. 3):1.
9. Buttermann, K. (1958) Clearance studies in normal and pathological pregnancy, with a critical evaluation of the methods. Arch. Gyn. Munch, 190:493. Chesley, L.C. and Sloan, D.M. (1964) 10. The effects of posture on renal function in late pregnancy. Am. J. Obstet. Gynecol., 89:754.
11. Crowe, L.R., and Hatch, F.E. (1977) Evaluating renal function. Postgrad. Med., 62:58-67. 12 Davison, J.M. and Hytten, F.E. (1974) Glomerular filtration during and after pregnancy. Brit. J. Obstet. Gynaecol., 81:588.
12. Dignam, W.J., Titus, P. and Assali, N.S. (1958) Renal function in human pregnancy. 1. Changes in glomerular filtration rate and renal plasma flow. Proc. Soc. Exp. Biol., 97:512.
13. Doolan, P.D., Alpen, E.L. and Theil, G.B. (1962) A clinical appraisal of the plasma concentration and endogenous clearance of creatinine. Am. J. Med., 32:65.
14. Dunlop, W. (1976) Investigations into the influence of posture on renal plasma flow and glomerular filtration rate during late pregnancy. Br. J. Obstet. Gynaecol., 83:17.
15. Edwards, K.D. and Whyte, H.M. (1959) Plasma creatinine level and creatinine clearance as tests of renal function. Aust. Ann. Med., 8:218.
16. Gylling, T. (1961) Renal haemodynamics and heart volume in normal pregnancy. Acta Obstet. Gynecol. Scand., 401, (Suppl. 5.):1.
17. Henry, R.J., Sobel, C. and Segalove, M. (1956) Tur-bidimetric determination of proteins with sulfosalicylic and trichloracetic acid. Proc. Soc. Exp. Biol. Med., 92:748.
18. Hytten, F.E. and Leitch, I. The Physiology of human pregnancy 2nd ed. Oxford. Blackwell scientific publications, 1971, pp. 132-64.
19. Jones, E.J. and Singer, B. (1978) Influence of angiotensin on regulation of glomerular filtration rate in the cat. Proc. Physiol. Soc. March, 40-41 P.
20. Karim, R.W., Harris, J.E., Beydoun, S.N. and Cuenca, V.G. (1976) Endogenous creatinine clearance during pregnancy. Obstet. Gynaecol., 48:239.
21. Kingsley, G.R. (1939) The determination of serum total proteins, albumin, and globulin by the Biuret reaction. J. Biol. Chem., 131:197.
22. MacGillivary, I. and Tovey, J.E. (1957) A study of the serum protein changes in pregnancy and toxaemia, using paper strip electrophoresis. J. Obstet. Gynaecol. Br. Epice, 64:361.
23. Robertson, E.G. (1969) Oedema in normal pregnancy. J. Reprod. Fert. Suppl., 9 (Suppl.):27.
24. Sirota, J.H., Baldwin, D.S. and Villarreal, H. (1950) Diurnal variations of renal function in man. J. Clin. Invest., 29:187.
25. Sims, E.A.H. and Krantz, K.E. (1958) Serial studies of renal function during pregnancy and the puerperium in normal women. J. Clin. Invest., 37:1764.
26. Smith, H.W. The kidney; structure and function in health and disease. New York, Oxford University Press 1951, p. 8.
27. Sohar, E., Scardon, E. and Levitt, M.F. (1956) Changes in renal haemodynamics during normal pregnancy. Clin. Res. Proc, 4:142.
28. Tobias, G.J., Md.aughlin, R.F. Jr. and Hopper, J.Jr. (1962) Endogenous creatinine clearance. N. Engl. J. Med., 266:317.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: