
Ali A. Qazilbash ( Department of Medicine, Khyber Medical College, Peshawar. )
June 1982, Volume 32, Issue 6
Original Article
Abstract
One hundred cases of hypertension were investigated and treated with Prazosin alone, Prazosin with a diuretic and Prazosin, Diuretic and a Beta-adrenergic blocker. They were followed up for two and more than two years. Prazosin was found to be very safe and effective antihypertensive drug either alone or in combination with a Diuretic, or Beta-adrcnergic blocker in various grades of hypertension. Average fall of blood pressure on standing was 32.92 systolic and 22.27 diastolic. Side effects were mild and only five patients had to stop taking their drug. Prazosin was specially found quite safe antihvpertensive drug in hypertension with uraemia (JPMA 32:135, 1982).
Introduction
Evergrowing importance of hypertension is reflected from the epedemiological studies. Nearly 20% of the population in America is suffering from hypertension (Page and Sidd, 1972). In Karachi, it has been reported in 12.4% of the population in a community (Abbasi and Syed, 1966). Recent survey in a European population has shown, that between 10 to 15% of adults are suffering from high blood pressure. Incidence of hypertension is low in developing countries. It is uncommon in certain African countries (Donnison, 1929). In Libyans it was 3% of the total medical admissions (Qazilbash, 1977). Modest rise of blood pressure is associated with 76.4% higher death rate in middle age, while the treatment ot hypertension has reduced the death rate from 55% to 18%.
Various drugs have been used for the treatment of hypertension either alone or in cornbination with other antihypertensive drugs, but uptill now no satisfactory (Irug with all the ideals has been discovered. In most of the patients with primary hypertension high peripheral vascular resistence is the cause of elevated arterial pressure, cardiac output is usually within normal limits, although it may he initially elevated. Arterial pressure can be lowered either by decreasing cardiac output or by decreasing peripheral resistence. Prazosin Hydrochloride is an alpha-ádrenoreceptor blocker. It lowers the blood pressure by relaxation of arteriolar smooth muscles, leading to reduction of total peripheral resistence, this blockade appears to be post-junctional, which explains the absence of tachycardia and release of Renin. Prazosirt has also been reported to reduce cholesterol (Oliver et al., 1978), and Cholesterol fraction in low density lipoproteins and very low density lipoproteins (Leren et al., 1980).
A trial of Prazosin (Minipress) was starteu in April 1978 and 120 cases of hypertension were studied, twenty cases (17%) were excluded because of various reasons.
Material and Methods
One hundred and twenty patients with high blood pressure were admitted in medical unit at Khybcr Hospital, Peshawar. All these cases, were assessod clinically, detailed history was taken and a thorough clinical examination was conducted including fundoscopy. Blood pressure was recorded daily in the morning and evening, both the in lying and standing position with a standard murcury syphygmomanometer for three days, standing blOOd pressure was recorded at least 2 minutes after standing. Fifth phase of Korotkov was taken as diastolic reading. During these three days,, all the laboratory investigations which included routine blood count, Urine examination on three different occasions, blood urea, serum creatinine, fasting blood sugar, creatinine clearance, serum cholesterol, triglycerides, total lipids and electrolytes were done, ECG was recorded in each patient.
Radiological investigation included chest X-ray, plain X-ray, Abdomen, and I.V.P. Renal Scan was done in those patients whose blood urea was above 100 mg percent and in some renogram was also performed.
Prazosin was started ofl the 4th day. Fifteen patients (12.5%) did not report for followup. So were dropped and five patients (4%) stopped taking drug due to side effects which was thought to be probably due to prazosin. Hundred cases have been followed for a minimum period of 2 years and some more than 2 years.
Results
Age and Sex:
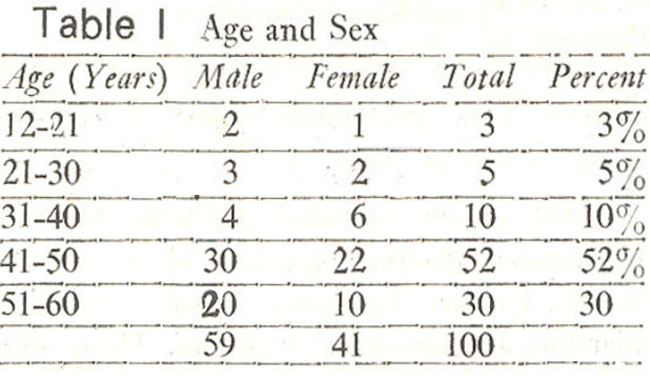
Table I shows the Age and Sex distribution in 100 patients.
Grades of Hypertension:
Fifty four patients had moderate hypertension (54%), twenty six (26%) mild and 20 had severe hypertension (20%) (Table II).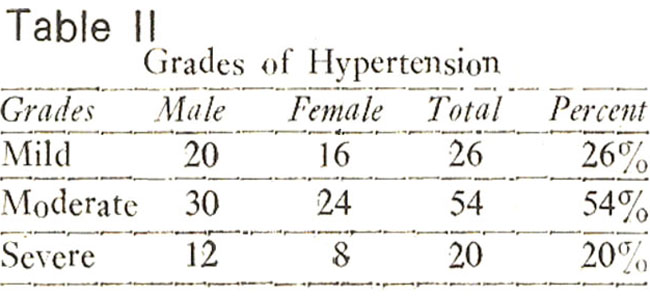
Type of Hypertension:
Eighty two patients had essential hypertension while 18 had secondary hypertension, ten were diabetic, four had pyelonephritis. Two had Glomerulone phritis. One coarctation of aorta, and cne had Cushings disease (Table III).
Retinopathy:
Seventy patients (70%) had grade II Retinopathy while twenty had grade I (20%) and 5 each had grade III and IV.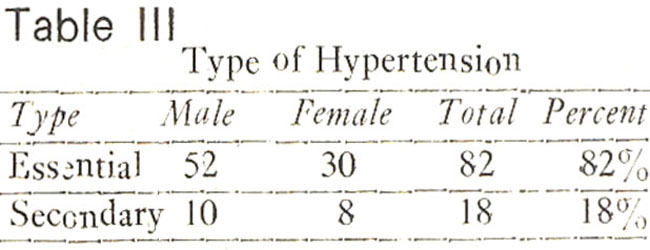
Laboratory Investigation:
Twenty six patients had high blood urea, with high creatinirie levels. 14 of them had blood urea above 100 mg%, Serum Cholesterol was high in 52 patients and hlocd sugar In 10 cases.
Urine examination was done thrice in each patient. Every patient had urine culture done. Thirty cases had positive urine culture, E. Coli being the commonest organism isolated.
Sixty two patients (62%) had E.C.G. abnormality of left ventricular hypertrophy, of these 40 were males and 22 females. Radiological studies of chest showed enlarged heart in 36 patients 24 of these were males and 12 females. IX.P. was done in all cases with normal blood urea.
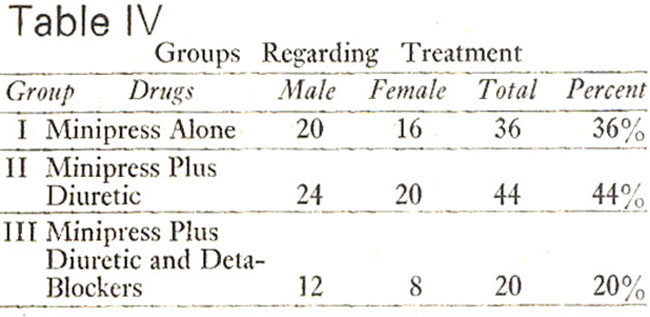
For treatment patients were divided into three groups (Table IV). Group I included 36 patients whose blood pressure was controlled with prazosm alone. In group IT, 44 patients required addition of a diuretic with prazocin to control the blood pressure. Twenty patients in group III were treated with prazosin, diuretic and beta-ad renergic blocking agents.
Discussion
Our findings indicate that Prazosin used alone or in combination with other antihypertensive agents is effective to reduce the blood pressure to normal levels. It is well tolerated and there is quite an appreciable fall. In supine as well as standing blood pressure, in supine posture fall of pressure on an average was 32.56 in systolic and 19.83 in diastolic pressure. In standing posture the fall in systolic pressure was 32.92 aad in diastolic pressure it was 22.27. Similar improvement has been reported by Stokes and Weber (1974), Hayes etal. (1976), Garden Stokes et al. (1975). We found Prazosin to be quite effective either alone or with a diuretic in mild and few moderate hypertensives, which has also been reported by LundJohansen (1974), Venables and Duff, (1974) and Bolzano (1974), Adriaensen and Vryens (1975), Rougier et al. (1974) Turner et al. (1975).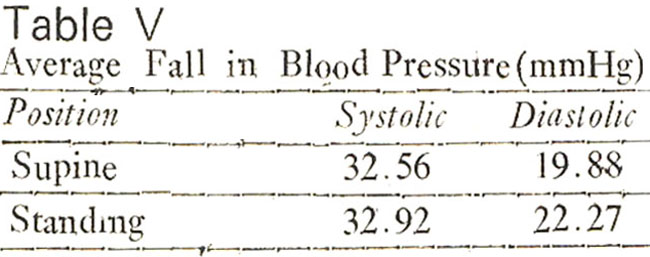
Our experience has not been encouraging with Prazosin alone or with a diuretic in some cases of moderate and most of the severe cases of hypertension. We used mostly either frusamide or Aprinox as a diuretic. In such cases a beta-adrenergic blocker Propranalol was added to the treatment. These patients were already taking 12 to 16 mg of Prazosin in divided (loses and a diuretic once or twice a day. Addition of beta-blocker in these eventually controlled the blood pressure. Successful control of blood pressure by combination of Prazosin and beta blocker has also been reported by Sanner Stedt et al. (1972), Zacest (1972), Gotlieb et al. (1972), Gorden et al. (1974), Koch-Weser (1974), Kincaid-Smith et al. (1975), Bolli and Simpson (1975), Turner et al. (1975).
High blood urea was recorded in 26 patients, 14 of these had a blood urea of over 100 mg%. In these cases we found Prazosin to be quite safe drug in lowering the blood pressure. without further deterioration in the kidney function. 8 oUt of 26 cases with high blood urea died (31%). In these patients we noticed progressive fall in the blood pressure with a gradual fall in blood urea and Creatinine Ievels and also improvement in kidney function. Comparatively small close of prazosin, was required in such cases. Effective use of prazosin in hypertens:on Diaslolic with Ureamia has also been reported by Curtis and Bateman (1975), Hayes et al. (1974), Pitts (1975).
First dose phenomenon as reported by Hayes et. al. (1976) and Kincaid Smith et al. (1975) with Prazosin was also noted by us, in two of our patients. Postural hypoten sion was recorded in 5 patients. In such cases the dose of Prazosin was gradually increased without any further attacks. This phenomenon was not noticed again once the first dose was started before going to bed at night.
Side effects recorded during the trial of Prazosin with or without diuretics were postural hypotension, dizziness specially while travelling. Some patients complained of headache, loose bowels. Urinary frequency, lassitude, excessive sleep, dryness of mouth, nausea, vomiting, diarrhoea and menstrual irregularity. These side effects were in general mild and they gradually disappeared on reassuring the patient and none of them stopped taking their drug.
Five patients stopped taking Prazosin because of side effects, three complained of tachycardia, one patient developed anginal type of chest pain and one lady teacher developed frequent extrasystoles giving her unpleasant feeling.
Acknowledgement
My thanks arc to Pfizer (Pakistan) Limited for financing the Project for one year and to Mr. Fazal-e-Wahid and Mr. Mushtaquc for typing facilities.
References
1. Abbasi, A.S. and Syed, S.A. Lt. Col. (1966) Atherosclerosis and coronary heart disease in Pakistan. Paper read at BMA-PMA meeting held in Karachi-December.
2. Adriaensen, H. and Vryens, R. (1975) Prazosin in hypertension. Practitioner, 214:268.
3. Bolli, P. and Simpson, F.O. (1974) Preliminary clinical trial of prazosin. A new oral antihypertensive agent. N.Z. Med. J., 79 :969.
4. Bolzano, K. Prazosin, A new Quinazoline, Derivative in the treatment of essential hypertension. In Prazosin, Evaluation of new antihypertensive agent. edited by D.W.K. Cotton. Excerpta Medica, 1974, 143.
5. Bolli, P. and Simpson, F.O. (1975) A new vasodilator drugs for hypertension. Br. Med. J., 3:637.
6. Cohen, B.M. (1970) Prazosin hydrochloride (CP-12, 229-1) an oral anti-hypertensive agent; preliminary clinical observation in ambulatory patients. J. Clin. Pharmacol., 10:408.
7. Curtis, JR. and Bateman, F.J.A. (1975) Use of prazosin in management of hypertension in patients with chronic renal failure and renal transplant recipients. Br. Med. J., 4:432.
8. Donnison, C.P. (1929) Blood pressure in the African native: its bearing upon the etiology of hvperpesia and arteriosclerosis. Lancet, I :6.
9. Gotlieb, T.B., Katz, F.H. and Chidsey, CA. (1972) Combined therapy with vasodilators and beta-adrenergic blockade in hypertension. A comparative study of minoxidil and hvdrallazinc. Circulation, 45:571.
10. Hayes, J.M., Graham, R.M. and O’Connell, B.P. (1974) Prazosin, in hypertension. Br. Mcd. J., 4:108.
11. Hayes, J.M., Graham, R.M., O’Connell, B.P., Muir, M.R., Speers, E. and Humphery, T.J. (1976) Experience with prazosin in the treatment of patients with severe hvperten-sion. Med. J. Aust., 1:562.
12. Koch-Wescr, J. (1974) Vasodilator drugs in the treatment of hypertension. Arch. Intern. Med.,133:1017.
13. Kincaid-Smith, P., Macdonald, I.M., Hua, A., Layer, M.C. and Pang, P. (1975) Changing conceports in the management of hypertension. Med. J. Aust., 1:327.
14. Leren, P., Foss, P.O., Hclgeland, A., Hjermann, I., Holme, I. and Lund-Larsen, P.G. (1980) Effect of pro-penelol and Prazosin on blood Lipids. The Oslo study.Lancet, 2:4.
15. Lund-Johansen, P. Haemodynamic changes at rest and during excercise. In long term prazosin therapy, in essential hypertension. In prazosin. Evaluation of a new Anti-hypertensive agent. Edited by D.W.K. Cotton excerpta medical, 1974, 43.
16. Oliver, M.F., Heady, J.A., Morris, N.J. and Cooper, J.A. (1978) Co-operative trial in the primary prevention of ischemic heart disease using clofibrate. Br. Heart J., 40:1069.
17. Page, L.B. and Sidd, j.j. (1972) Medical management of primary hypertension. N. Engi. J. Med., 287:960.
18. Pitts, N.E. (1975) The clinical evaluation of prazosin, a new antihypertensive agent. Postgrad. Med. Spec., 117.
19. Qazilbash, A.A. Cardiovascular disease in Libyan’s paper read at 3rd Cardiac congress of Pakistan 1977,
20. Richardson, D.W., Ramaswamy, D. and Ramirez, A. (1968) Effect of prazosin on arterial pressure and cardiac output in human hypertension. Circulation, 38:164.
21. Rougier, M., Lahon, 1I.F.J. and Cini, AR. (1974) Prazosin new antihypertensive agent. Br. J. Clin. Prac., 28:281.
22. Stokes, G.S. and Weber, M.A. (1974) Prazosin, preliminary report and comparative study withother antihvpertensive agents. Br. Med. J.; 2:298.
23. Sanner-stedt, R., Stenberg, J. Vedin (1972) A Chronic beta adrenergic blockade in arterial hypertension. Hemodynamic influences of hydrilazine and dynamic exercise and clinical effect of combined treatment. Am. j. Cardiol.,718.
24. Turner, AS., Watson, O.F. and Peel, J.O. (1975) Clinical experience with Prazosin in hypertension. Postgrad. Med. Spec., No. 88.
25. Venables, T. and Duff, R.S. (1974) A comparative trial of Prazosin and Methy L dopa. Prazosin, Evaluation of a new antihypertensive agent. Edited by D.W.K. Cotton excreptor medic. III.
26. Zacest, R., Gilmore, E. and Koch-Weser, J. (1972) Treatment of essential hypertension with combined vasodilation and beta-adrenergic blockade. N. EngI. J. Med., 286:617.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: