
Tariq Mufti ( Department of Surgery Ayub Medical College, Abbottabad. )
May 1983, Volume 33, Issue 5
Case Reports
Abstract
Four cases of intracranial Echinococcosis presenting in Department of Neurosurgery, Jinnah Post graduate Medical centre, Karachi over the period of years are reported along with their follow-up to date. Special aspects of pathogenesis and treatment of the disease is discussed in order to establish early diagnosis and proper management of disease (JPMA 33:115) 1983).
Introduction
Human infestation with hydatid disease once thought to be limited to certain geographical zones of the world is now recognised as of global distribution; however, its frequency rises markedly in sheep raising sectors. Intracranial hydatidosis occupies only a small fraction of the total incidence i.e. less than 2-3% (Katz and Pan, 1958; Cole, 1947; Jidejian, 1953; Magath, 1950) yet need for its urgent and accurate diagnosis followed by prompt and proper management surpasses the disease situated in most other locations of the body. The fact that the disease is benign and curable with proper management carried out in time is to be kept in mind.
Case reports
Case I: A 14, years old female, from rural Punjab settled in Karachi was admitted on 21st Nov. 1970 with two years history of intermittent attacks of headache, vomiting and involuntary movements of left upper extremity. She developed progressive left hemiperesis, urinary incontinence and drowsiness. On examination apart from drowsiness and left hemiperesia patient had evidence of hydrocephalus, loss of upward gaze and bilateral papilloedema. X-ray skull showed changes due to raised intracranial pressure, and high voltage, irregular slow activity; EEC was obtained over right temporoparietal region. Air ventriculogram through biparietal burr holes revealed most remarkable and pathognomonic picture of hydatid disease (Fig. 1).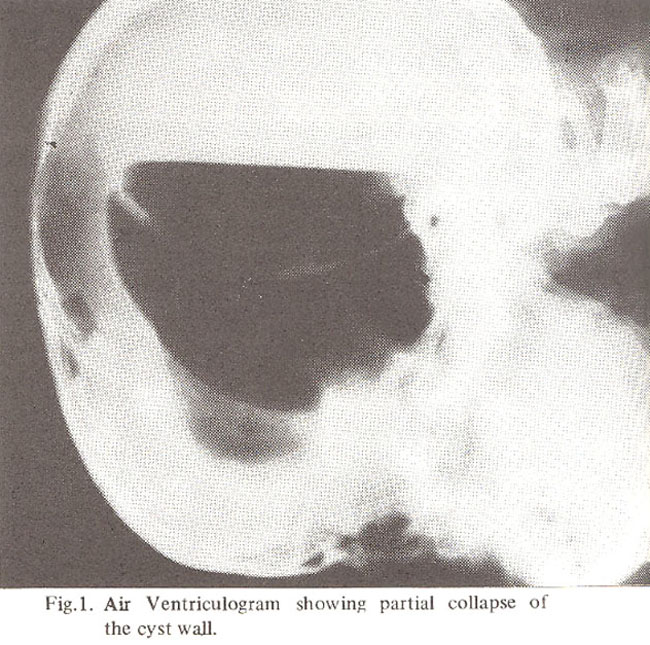
Operation was carried out immediately following ventriculography and a solitary mother cyst from right parieto-temporal region was removed in toto. Little spillage of the hydatid fluid could not be avoided. However cavity was washed with Hydrogen peroxide solution. Complete neurological recovery was obtained with in a week following the operation.
After remaining well for about six months patient had relapse of headache, vomiting and epileptic fits. She was readmitted on 14-5-1971 in semiconscious state and was reexplored through previous wound when a small daughter cyst sitting on the top of a large cyst containing yellow fluid and hydatid sand was removed. Pericyst which was left in situ during last operatiJn was also removed in toto. Recovery of the patient was slow and she expired due to cardio-respiratory failure a week after operation.
Case 2: A 9 years old male from Karachi was admitted with complaints of intermittent headache, vomiting and low grade fever of over one year duration. In addition there was progressive loss of visual acuity and left hemiperesis of recent onset. He was brought in Hospital due to sudden deterioration of conscious state. He exhibited horizontal nystagmus on examination with dilated and slow reacting pupils and left hemiperesis. Significant positive findings on investigations were, Eosinophiia (7%), decreased radioisotope uptake in right cerebral hemisphere and angiographic evidence of right fronto-parietal ;pace occupying lesion. Patient was operated upon mmediately and 15 cm diameter hydatid cyst i:ontaining slightly turbid fluid later proved to be infected was removed. Fibrous pericyst was also removed. Recovery of the case was complicated by development of jaundice and meningitis postoperatively. Cystic hygroma formation was an added misfortune. However, patient eventually fought his way to satisfactory recovery with minimal residual neurological deficit and was discharged home.
Three months later patient was readmitted with severe hydrocephalic attacks. Ventricular tap confirmed the diagnosis of hydrocephalus (Postmeningitis). Ventriculoperitoneal shunt was inserted immediately. Patient eventually died after a few weeks due to intercurrent infections.
Case 3 : A 22 years old tailor, resident of Karachi, was admitted on 12.4.1982 with complaints of headache, vomiting and jacksonian type of epileptic fits limited to left upper extremity for over 6 months duration and progressive left hemiperesis appearing three weeks prior to admission. Examination revealed bilateral papilloedema in addition to left hemiperesis. Total and differential leucocytic counts including Eosinophils were within normal limits. Brain scan with Tc 99 could not discover any lesion. However, slow wave pattern in right fronto-parietal region on EEG and an avascular spherical area in right carotid angiograrn were conclusive of a space occupying lesion. Operation on the patient through a frontoparietal flap revealed solitary intracerebral hydatid cyst in right cerebral hemisphere in the region of frontoparietal lobe which was confirmed by needle aspiration. 10% formaline was injected in the cyst through the same needle. 6.5 cm diameter cyst was removed in toto without spillage. No definite pericyst could be isolated. Pathology report confirmed the clinical diagnosis. Patient showed complete reversal of papilloedema and neurological deficit. Mebendazole tablets 1000 mg 6 hourly was given to the patient for three months and then reduced to 500 mg QI.D. for next 6 months. Patient has resumed his profession with full efficiency and there is no evidence of recurrence to date. Live scan, X-ray chest, I.V.P. and other investigations to fmd same pathology elsewhere in the body proved negative.
Case 4 : A 10 years old boy from Karachi was admitted on 14.12.1978 with history of intermittent attacks of headache and generalised epileptic fits. Examination revealed papilloedema but not other abnormal neurological findings. Total leucocytic count was raised to 22000 with eosinophils 3% of total. Decreased uptake to Tc 99 in left frontal region was detected on scan. Carotid angiography endorsed the diagnosis of space occupying lesion in this location. On explora-tion a solitary ruptured hydatid cyst without significant evidence of pericyst formation was found. Cyst was removed and diagnosis was confirmed histopathologically. Smooth postoperative recovery and complete reversal of neurological signs for three years was noted.
He was readmitted in May 1982 with recurrent symptoms of headache, vomiting and progressive right hemiperesis with mild dysphasia. Carotid angiography revealed recurrence of a large lesion in left parietal area with a calcified pericyst. On operation multiple small cysts of varying diameters in addition to a large one were found within a hard shell of calcified pericyst (Fig. 2).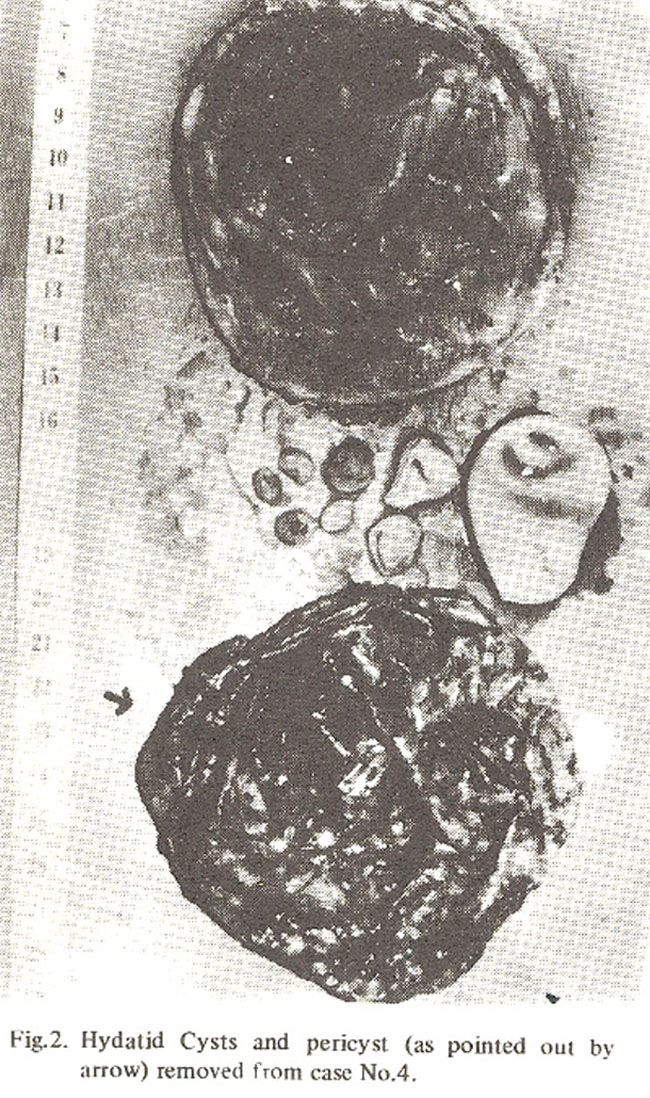
Large cyst was dealt with as in case 4. Pericyst was removed with some difficulty. Although patient made full recovery of previously existing neurological deficit; however, persistent and resistant Staphylococcal infection leading to meningitis and septicaemia proved fatal six weeks postoperatively.
Discussion
Exact worldwide incidence of intracranial hydatid disease has not yet been evaluated. A study from North America on the incidence of Echinococcosis (Katz and Pan, 1958) from 1900 - 1958 describes only six cases of intracranial disease out of a total of 541 cases with an incidence of 1%. Australasian hydatid registry gave figures of 0.9% out of 1802 cases while in another study it was 2.1% (Dew, 1928). Douglas (1948), Jidejian (1953), Schlanger and Schianger (1948) have not mentioned the intracranial location of this disease. 5% incidence was reported in one study (Greenfield, 1971).
There is only one such report from Pakistan (Rehman, 1980) mentioning five cases dealt with in Lahore Neurological centre. Another case has been reported from Multan (Raja, 1982). Therefore, a total of 10 cases including those presented in this paper and perhaps a few more missing from being recorded give us an indication of significantly higher incidence than figures quoted in western literature.
It is only Echinococcus Granulosis which forms cysts intracranially, out of all the four species of Echinococcus affecting human beings. According to the mode of infestation two different types of the disease are recognised, Embryonal and Scolecal. Former is more frequent in which embryo after entry through intestinal mucosa escapes the barriers of mesenteric lymphatics, liver and lung enters general systemic circulation and infests the brain or coverings. This mode sometimes is known as primary hydatidosis. Cysts are usually solitary, mostly occurring in children, and are rapid and extensive. in development (as in our cases 3 & 4). Their prognosis after removal is usually satisfactory. If left untreated most of the patients die within four years after diagnosis. Scolecal type is due to scoleces escaping from ruptured cysts elsewhere and metastasising as multiple, slowly developing cysts intracranially (eleven years old disease was described by Ayres et al. in 1963). Their postoperative prognosis is more guarded. Usually site for the cysts is stipratentorial compartment, nevertheless, there are occasional reports of subtentorial cerebellar cysts (Abbasioun, 1978; Rehman, 1980). Area of distribution of middle meningeal artery is most vulnerable site (Danziger and Bloch, 1975). Cysts begin usually a few millimeter deep in cortical tissue and press on surrounding brain. Bluish dome of the cyst is frequently visible from the surface after incising the dura.
Undoubtedly C.T. scan is the best indicator of the pathology out of all radiological and radioisotopic investigations available to date (Abbasioun, 1978) which shows a sharply defined, spherical cystic lesion with none or negligible rim enhancement and absence of perifocal oedema. Cerebral angiography outlining an avascular circular area with stretching of surrounding vessles and a negative brain scan showing an area of silence in suspected cases provides enough grounds for diagnostic aspiration through a burr bole, If clear fluid is aspirated then the air cystogram may show the pathognomonic picture of partially collapsed wall of the germinal layer of the cyst. Definitive procedure is carried out immediately after obtaining air cystographic proof in order to avoid spillage of the hydatid fluid.
Casoni intradermal test is not always positive and is considered nonspecific. Similarly eosinophilia is met uncommonly and cannot be relied upon. Recently more specific serological tests have been introduced (Kupp and Chalton, 1982). Finding are-5 in the immunoelectrophoresis is an important break through in diagnosing the pathology. Furthermore, disappearance of this component within one year post-operatively gives good indication of complete cure.
Long term use of Mebendazole and Fluomemendazole for checking the progression of cysts and in some cases regression of the cysts have been documented. However, intracranial disease, due to its peculiar location has to be treated surgically. Mebendazole or fluomebendazole can be used preoperatively or during recurrence. Its use postoperatively may help in reducing the incidence and recurrence. Various techniques have been described to remove the cyst in toto (Arena and Julani, 1955; Gripgnissiotis, 1957), but in the experience of this centre simple and cautious manouvering of partially collapsed cysts with plain dissecting forceps is good enough’Removal of the pericyst is necessary only if it is well formed fibrous or calcified layer.
Acknowledgement
I am highly indebted to Professor I.H.Bhatti Head of Neurosurgical Unit, J.P.M.C. for allowing me to use the records of his Department and letting me describe cases as well as guiding me in preparation of this article. I must pay my gratitude to Professor Iftikhar Raja, Head of Department of Neurosurgery, Nishtar Medical College, Multan for providing valuable information from the record of his department.
References
1. Abbasioun, K. et al. 1978) Computerized tomography Hydatid cysts of the brain. J. Neurosurg., 49 (3) : 408.
2. Arena, Iniguez, R. and San, Julian, J. (1955) Hydatid cysts of Brain. J. Neurosurg., 12 : 323.
3. Ayres, C.M. et al. (1963) Cerebral Hydatidosis. Clinical case report with a review of pathogenesis. J. Neurosurg., 20 : 371.
4. Cole, G. (1947) Australasian Hydatid Registry. Trop. Dis. Bull., 44 :6.
5. Danziger, J. and Bloch, S. (1975) Tapeworm cyst infestation of the brain. Clin. Radial., 26 : 141.
6. 6. Dew, H.R. (1928) Hydatid disease. Its pathology, diagnosis and treatment. The Australasian Medical publishing Company Ltd., Sydney. p.429.
7. Douglas, D.M. (1948) Hydatid disease. Edinb. Med. J.,55 :78.
8. Greenfield (1971) Neuro Pathology, Edward Arnold Publishers, 2nd Ed. p.220.
9. Relunan, N.U. (1980) Hydatid disease of the central nervous system. Garyounis Med. J., 3 : 81.
10. Gripgnissiotis, B. (1957) Hydatid cyst of the brain and its treatment. Neurology, 7: 789.
11. Jidejian, Y. (1953) Hydatid Disease. Surgery, 34 : 155.
12. Katz, AM., and Pan, C.T. (1958) Echinococcus disease in the United States. Amer. J.Med., 25 : 759
13. Kupp, M.A. Chalton, M.T. (1982) Current Medical Diagnosis and Treatment, Lange Medical Publications, California. 1982 Ed. p.895.
14. Magath, T.B. (1950) Present status of hydatid (echinococcus) disease in North America. Arch. Int. Hydatid., 11: 193.
15. Raja, I. (1982) Personal Communication.
16. Schlanger, P.M. and Schianger, H. (1948) Hydatid disease and its roentgen picture. Amer. J. Roentgenol., 60 : 331.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: