
Nadeemullah Khan ( Departments of Medicine and Surgery, The Aga Khan University Medical College, Karachi )
Hasanat Sharif ( Departments of Medicine and Surgery, The Aga Khan University Medical College, Karachi )
Saqib Hamid Qazi ( Departments of Medicine and Surgery, The Aga Khan University Medical College, Karachi )
Junaid A. Razzak ( Department of Emergency Medicine )
January 2005, Volume 55, Issue 1
Short Communication
Abstract
Objective: To review the incidence, clinical presentation and outcome of Non traumatic Aortic emergencies in a tertiary care hospital and its evaluation in the Emergency department (ED).
Methods: We conducted a retrospective review of cases presented to the ED at Aga Khan University Hospital during 15 year period (1988 - 2002) who had final diagnosis of Aortic Dissection or Ruptured Aortic Aneurysm. Patients without confirmatory investigations were excluded. We aimed at looking for the incidence, clinical presentation, evaluation in the ED and final outcome.
Results: Of the 12 cases, 7 had aortic dissection while the remaining 5 had ruptured aortic aneurysm. For Aortic dissection, mean age of presentation was 53 years with male predominance. Most of these patients had chest pain. Most common comorbid condition was hypertension. Pulse deficit was found in 2 cases, murmur in 4 cases, and focal neurologic deficit in 2 cases. Electrocardiogram revealed ischemic changes in 3 cases. Widened mediastinum on chest x-ray was present in all cases. The only initial misdiagnosis was cardiac ischemia. One patient survived to discharge. For patients presenting with ruptured aortic aneurysm, mean age of presentation was 52 yrs with a male predominance. The associated comorbid condition was hypertension. Almost all patients presented classically with abdominal pain, hypotension and palpable mass. No patient survived to discharge.
Conclusion: Aortic emergencies although rare, are associated with significant mortality. High index of suspicion and prompt recognition by the emergency physician is of key importance (JPMA 55:6;2005).
Introduction
Non traumatic Aortic emergencies, including Aortic dissection and ruptured Aortic aneurysm, are rare but potentially lethal diseases. High index of suspicion on part of the treating physician, prompt diagnosis and expedient management are essential for successful patient outcome. However, clinical diagnosis of these conditions can be extremely challenging in best of the circumstances. According to some estimates, as many as one third of aortic dissections are never diagnosed.1 Also, the incidence may vary in various populations depending upon the prevalence of risk factors like untreated hypertension, advanced age and diseases of aortic wall.1-4 Studies have reported estimated incidence of aortic dissection up to 5-30 cases per million people per year.4
Although an aneurysm may be complicated by dissection these are two different entities. An aortic aneurysm is a sac formed by the dilatation of the arterial wall. An aortic dissection, on the other hand, is the splitting within the medial layer of the artery caused by bleeding within the arterial wall. Mortality related to missed aortic emergency far surpasses that associated with missed myocardial infarction.5
Although originally described in 1761 by Morgagni6 and officially named "Aneurysme dissequent" by Lannaec in 1819, the clinical recognition of disease has been very slowly developing.1,2
A recent study showed that emergency physician\'s suspected an aortic dissection in 19 of the 44 patients, only 43% that presented with an aortic dissection. Most of these dissections seemed to be acute by symptomatology.5 In another study the diagnosis of aortic dissection was missed in 38% of cases on initial evaluation and in up to 28% of cases the diagnosis was first established at the post mortem examination.4 Also many patients with aortic dissection die before their presentation to a hospital or prior to diagnosis.4 Although the symptoms of aortic dissection may mimic myocardial ischemia which is a more common entity in the emergency setting, the institution of thrombolytic therapy in such cases requires exclusion of aortic dissection as one of the absolute contraindication to thrombolytic therapy.7
Rapidity of diagnosis and institution of appropriate treatment is paramount to the patient\'s survival as incremental mortality is 1% per hour.8 Although sophisticated technologies are available for rapid and accurate diagnosis of Aortic dissection, a high index of suspicion by the physician is still the single most important factor in making the diagnosis.1-4
Similar to aortic dissection, the rupture of an abdominal aortic aneurysm is a catastrophic event with a uniformly fatal outcome if untreated. Up to 62% of patients die before reaching the hospital. The overall mortality rate after rupture may exceed 90%.9 The incidence of abdominal aortic aneurysm appears to be rising and this is partly explained by an aging population.9 Like aortic dissection, it is more common in elderly males. Other risk factors include positive family history, and associated comorbid condition like obstructive pulmonary disease and peripheral vascular disease.9,10
Ruptured abdominal aortic aneurysm, is diagnosed classically by the triad of abdominal or back pain with hypotension and a palpable mass, but unfortunately this triad is only present in 50% of patients.9,10 There are also various atypical presentations described in the literature including ureteric colic, painful femoral neuropathy, unexplained high output cardiac failure, unexplained gastrointestinal bleeding and massive hematuria. Clinical diagnosis is thus infrequently missed in the emergency room of even in the most advanced medical center.11 Consequently, appropriate treatment in the form of expeditious laprotomy and surgical repair is not achieved leading to possible avoidable mortality. Ruptured abdominal aortic aneurysm was misdiagnosed as cholelithiasis with cholecystitis in case of Albert Einstein, leading to his demise.12
There is limited literature from developing countries on these potentially lethal emergencies. One study carried out in India found 35 autopsied cases of aortic dissection over a period of 12 years.13 Two studies carried out in India looked at the role of Transesophageal echo and digital subtraction angiography for detection of aortic dissection.14,15 Another study looked at the surgical experience with dissecting and non dissecting aneurysms of aorta.16
The objective of this study was to review the incidence, clinical presentation and outcome of non-traumatic aortic emergencies in a tertiary care hospital and its evaluation in the emergency department (ED).
Methods
A case series of patients with the final diagnosis of aortic dissection or ruptured aortic aneurysm discharged from the Aga Khan University Hospital was conducted. Aga Khan University Hospital is a 450 bedded tertiary care hospital with an emergency center with a census of approximately 40,000 patients annually. The hospital is located in Karachi, Pakistan, a city with a population of approximately 14 million people.
The search for patients with an admission diagnosis of either aortic dissection or ruptured aortic aneurysm was carried out for the 15 year period (1988-2002). The search was done using the above key words using the hospital\'s information management system. The medical records of these patients were obtained and information was collected using a data collection instrument. Of these patients, we selected only those patients who had confirmed diagnosis of either aortic dissection or ruptured aortic aneurysm based on one of the imaging modalities. Patients with clinical suspicion of aortic dissection or Ruptured aortic aneurysm and died or left hospital before confirmatory investigations done, were excluded from final analysis. Data for the study patients were recorded on the questionnaire by one of the investigators and then rechecked for errors by the principal investigator. Data was entered and analyzed using SPSS statistical program. The study was in accordance with the ethical standards of Helinski declaration of 1975, as revised in 1983.
The aortic dissection was classified into acute or chronic types, depending on the duration of symptoms. Acute aortic dissection was diagnosed if the diagnosis was made within 2 weeks of onset of symptoms, and chronic aortic dissection was diagnosed if the symptoms were of more than 2 weeks duration. Stanford classification of aortic dissection was used. Type \'A\' being the one involving the ascending aorta regardless of the entry site location; and type B, involving the Aorta distal to the origin of the subclavian artery.
Results
Sixty cases were identified in which the admission diagnosis was either aortic dissection or ruptured aortic aneurysm. Of these, 12 patients had the final, confirmed diagnosis of aortic dissection or ruptured aortic aneurysm. Forty eight patients had a clinical suspicion but the diagnosis was not confirmed as the patient either died or left hospital against medical advice before confirmatory investigation or the diagnosis was excluded on investigation. Twelve cases were truly identified as either aortic dissection (7 cases) or ruptured aortic aneurysm (5 cases) in a period of 15 years.
Aortic Dissections
For aortic dissection mean age of presentation was 53 years with a range of 24-67 years. There was male predominance with the ratio of 2.5:1. Most of the patients (6/7), presented either with chest or epigastric pain with associated symptoms of shortness of breath and diaphoresis. One patient presented with only shortness of breath without chest pain. The duration of symptoms was prolonged in most cases with one person presenting 3 days after the symptoms started. More than half the patients (4/7) had a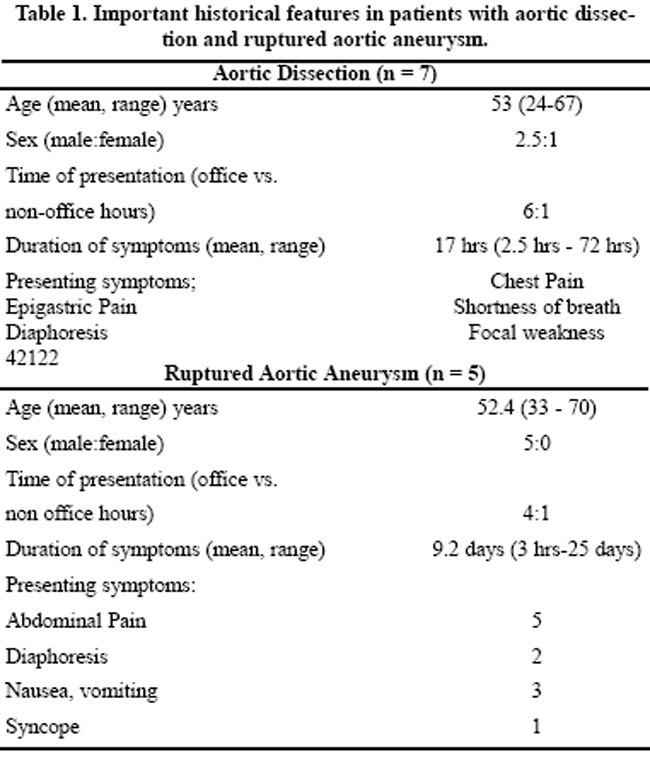
history of hypertension while one patient had Marfan\'s
syndrome.
Physical examination of these patients revealed a pulse in the range of 56-140 beats per minute. Elevated BP on presentation was found in only 2 cases. Pulse deficit was detected in 2 cases and absent in 2 cases while in the rest it was not documented. The difference of blood pressure in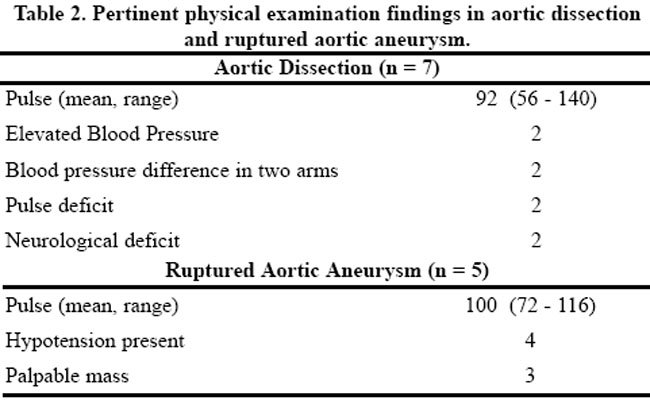
two arms was found in two cases while it was not documented in 3 cases. Cardiac examination was normal in 3 cases while systolic or diastolic murmur was heard in 4 cases. Focal neurological deficit was present in 2 cases and it was not documented in the rest.
The laboratory investigations including a complete blood count, electrocardiogram, chest X-ray and cardiac enzymes were performed and documented in all cases. Hemoglobin was found to be normal in all cases except one. Electrocardiogram revealed ischemic changes in 3 cases; including one patient with ST segment elevation, one patient with ST segment depression and one with T wave inversion suggestive of ischemia. Cardiac enzymes (CK and CKMB) were normal in all of these cases. Chest x-ray finding of widened mediastinum or soft tissue mass density in the mediastinum was present in all of the cases. The only initial misdiagnosis was cardiac ischemia (3/7) but none of the patients met the criteria for receiving thrombolytic therapy. The confirmatory investigations performed were CT scan in 3 cases, Aortogram in 2, Transthoracic echo in 2 and Transesophageal echo in 2 cases. In some cases more than one investigation was performed. Type A dissection was present in 6 cases.
Three patients were managed conservatively due to either high risk of surgery or refusal of surgery by patients or care-givers. One patient died in the ED before any intervention. Rest of the patients underwent surgery. Only one patient survived to discharge.
Ruptured Aortic Aneurysm
The mean age of the patients presenting with ruptured aortic aneurysm, was 52 years. All were male. Again there was a lot of delay in presentation to the emergency department with mean duration of symptoms around 9 days. Abdominal pain was present in all cases with associated symptoms of diaphoresis, nausea, vomiting and syncope with variable frequency. The physical exam findings were hypotension in 4 cases and palpable mass in 3 cases. The associated comorbid conditions included hypertension in 2 cases, chronic renal failure in 2 and chronic obstructive pulmonary disease and asthma in 2 cases. Two patients had no underlying comorbid condition.
The investigations performed included a complete blood count, ultrasound abdomen and CT scan abdomen. Haemoglobin was low in all cases. Aneurysm was detected in 3 cases with an ultrasound and in 2 cases with CT scan. One patient was high risk candidate for surgery and family agreed for conservative management. Four patients underwent surgery but did not survive till discharge.
Discussion
Both aortic dissection and ruptured aortic aneurysm are associated with significant mortality that mandates early identification and management.1-5, 8-10
Our series revealed only 12 diagnosed cases over a period of 15 years. This is probably due to under diagnosis of the condition. Three factors account for this difference. First, as there is no pre hospital care available in this part of the world and many cases die before reaching the hospital. Second, though we still see many patients in our emergency department, a large number of patients go to other hospitals. Third, many patients who are received dead on arrival or in cardiac arrest or expire in the emergency room before diagnosis, do not undergo autopsy to reveal the underlying cause.
Several features emerge from our study and from past reports that may be helpful in suggesting the diagnosis. As in other studies, we found that both diseases affect men more frequently than women with the incidence increasing with age.1,2,9,10,17-19 The duration of symptoms was prolonged in most of these cases, as in this part of the world people seek care from home remedies and other conventional methods of treatment before coming to the hospital. The late presentation leads to delayed diagnosis and worse outcome in these cases. Most of these cases presented during office hours with only two cases presented out of regular office hours. The possible explanation could be that during regular office hours expertise is available for improved diagnosis which might be limited during out of office hours leading to either missed diagnosis and discharge or death without diagnosis.
In our limited series we found that most of the cases have very classic presentation of both aortic dissection and ruptured abdominal aortic aneurysm. Literature reports various atypical presentations of these entities which are rare and likely to be missed.11
For cases with ultimate diagnosis of aortic dissection our series revealed that important predictive findings either were not checked or not documented in 50% of cases. These include pulse deficit, blood pressure difference in two arms and neurological deficit. In developing countries with limited resources, physicians have to rely on their clinical skills. This is especially true for physicians taking care of patients in emergencies. For aortic dissection, Vonkodolitsch et. al. devised a clinical predictor model for diagnosing aortic dissection based on history, physical and chest radiography findings.4 They identified three variables that enable identification of acute aortic dissection in 96% of cases. Thes are (1) chest pain with immediate onset, tearing or ripping in character, or both; (2) Pulse differentials, blood pressure differentials, or both and (3) Mediastinal widening, aortic widening, or both. The assessment of these findings identify 96% of acute aortic dissection cases. The probability of dissection is high (>83%) with isolated pulse or blood pressure differential, or combination of the three variables, intermediate with isolated findings of aortic pain (31%) or mediastinal widening (39%) and probability is low (7%) with the absence of all the three variables.4 Chest x-ray and electrocardiogram are two initial important screening investigations. A normal electrocardiogram in a patient with chest pain would make other conditions more likely. Similarly, chest x-ray not only helps to diagnose a widened mediastinum but also rules out other conditions like pneumothorax and pneumonia.
Late presentation of patients with ruptured abdominal aortic aneurysm leads to hypotension and shock state. These patients presented with the classic triad of abdominal pain, palpable mass and hypotension, which is a poor prognostic sign for survival even after timely diagnosis.20,21 Finally, effective therapy for these conditions requires awareness, high level of suspicion and prompt recognition.
References
1. Pretre R, Segesser L. Aortic dissection. Lancet 1997;349:1461-4.
2. Slater E, Desanctis W. The clinical recognition of dissecting aortic aneurysm. Am J Med 1976;60:625-33.
3. Crawford E. The diagnosis and management of aortic dissection. JAMA 1990;264:2537-41.
4. Khan I, Nair C. Clinical diagnostic and management perspective of aortic dissection. Chest 2002;122:311-28.
5. Sullivan P, Wolfson A, Leckey R, et al. Diagnosis of acute thoracic aortic dissection in the emergency department. Am J Emerg Med 2000;18:46-50.
6. Morgagni GB. Desedibus et Causis Morborum per Anatomen Indagatis Libri Quinque.Venetiis, ex typog Remondiuiana,1761. Ned Tijdschr Geneeskd 2001;145:2487-92.
7. Cummins R. ACLS provider manual. Dallas: American Heart Association, 2002, pp. 123-44.
8. Sarasin F, Louis-Simonet M, Gaspoz J, et. Al. Detecting acute thoracic aortic dissection in the emergency department: time constraints and choice of the optimal diagnostic test. Ann Emerg Med 1996;28:278-88.
9. Ernest C. Abdominal aortic aneurysm. N Engl J Med 1993;328:1167-72.
10. Vliet J, Boll A. Abdominal aortic aneurysm. Lancet 1997;349:863-6.
11. Banerjee A. Atypical manifestation of ruptured abdominal aortic aneurysms. Postgrad Med J 1993;69:6-11.
12. Chandler JJ. The Einstein sign: the clinical picture of acute cholecystitis caused by ruptured abdominal aortic aneurysm. N Engl J Med 1984;310:1538
13. Vaideeswar P, Deshpande JR, Sivaraman A. Aortic dissections: a pathologic study of 35 autopsied cases. Indian Heart J 1998;50:62-8.
14. Ansari A Transesophageal echocardiography. Indian Heart J 1993;45:227- 58.
15. Tyagi S, Prasad GS, Khalilullah M. Evaluation of aortic aneurysms and dissection of aorta by intravenous digital subtraction angiography. Indian Heart J 1990;42:55-7.
16. Bhan A, Choudhry SK, Saikia M, et al: Surgical experience with dissecting and non-dissecting aneurysms of the ascending aorta. Indian Heart J 2001;53:319-22.
17. Larson EW, Edwards WD. Risk factors for aortic dissection: a necropsy study of 161 cases. Am J Cardiol 1984;53:849-55.
18. Hagan P, Nienaber C, Isselbacher E, et al. The international registry of acute aortic dissection (IRAD): new insight into an old disease. JAMA 2000;283:897-903.
19. Spittell P, Spittell J, Joyce J, et al. Clinical features and differential diagnosis of aortic dissection: an experience with 236 cases. Mayo Clin Proceed 1993;68:642-51.
20. Sternbergh W, Gonz M, Garrard C, et al. Abdominal and thoracoabdominal aortic aneurysm. Surg Clin North Am 1998;78:827- 42.
21. Brimacombe J, Berry A. Haemodynamic management in ruptured abdominal aortic aneurysm. Postgrad Med J 1994;70:252-6.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: