
M. Naqi Zafar ( Zafar Research and Diagnostic Centre, Rimpa Plaza, MA. Jinnah Road, Karachi. )
Rakhshanda Baqai ( PMRC Research Centre, Basic Medical Sciences Institute, Jinnah Postgraduate Medical Centre, Karachi. )
Tariq Zia Lodi ( PMRC Research Centre, Basic Medical Sciences Institute, Jinnah Postgraduate Medical Centre, Karachi. )
Suha Ahmad ( PMRC Research Centre, Basic Medical Sciences Institute, Jinnah Postgraduate Medical Centre, Karachi. )
Waquar uddin Ahmed ( PMRC Research Centre, Basic Medical Sciences Institute, Jinnah Postgraduate Medical Centre, Karachi. )
Huma Qureshi ( PMRC Research Centre, Basic Medical Sciences Institute, Jinnah Postgraduate Medical Centre, Karachi. )
Sarwar J.Zuberi ( PMRC Research Centre, Basic Medical Sciences Institute, Jinnah Postgraduate Medical Centre, Karachi. )
Qamar Jamal ( Department of Pathology, Basic Medical Sciences Institute, Jinnah Postgraduate Medical Centre, Karachi. )
S. Mahmood Alam ( Department of Pathology, Basic Medical Sciences Institute, Jinnah Postgraduate Medical Centre, Karachi. )
April 1991, Volume 41, Issue 4
Original Article
ABSTRACT
To determine the frequency of giardiasis in patients undergoing upper G.l. endoscopy for dyspepsia and other upper G.I. disorders, duodenal aspirates were collected in 200 patients and simultaneous duodenal biopsies in 163 patients. Nine percent aspirates and 1.8% duodenal biopsies showed Giardia lamblia trophozoites. Giardiaas a cause of dyspepsia should be considered in patients with negative endoscopy and in those who remain symptomatic inspite of adequate treatment for known upper G.l. disorders (JPMA 41: 74, 1991).
INTRODUCTION
Giardia lamblia is a flagellated protozoan which resides in the upper part of the small intestine. The parasite has two forms vegetathre and cysts. Clinical manifestations of giardiasis are epigastric pain, dyspepsia, nausea, anorexia, foul explosive diarrhoea and abdominal cramps. Attempts should be made to isolate the trophozoite/cyst in the stool. If these are repeatedly negative and the symptoms persist, it is best to endoscope the patient, to exclude a peptic ulcer and simultaneously obtain duodenal aspirate, since Giardia lamblia have been seen in duodenal juice1 and finally to obtain a jejunal/duodenal biopsy for the detection of Giardia lamblia2. The aim of the study was to determine the frequency of giardiasis in patients undergoing upper G.I. endoscopy.
PATIENTS AND METHODS
Two hundred patients included in this study underwent endoscopy for one of the following complaints: Epigastric pain, dyspepsia, vomiting, heartburn/ water brash, dysphagia, weight loss, G.I. bleeding and for follow-up in duodenal ulcer, gastric ulcer, oesophageal varices and gastritis patients. Indications for endoscopy, endoscopic findings and other parameters were entered in a standard proforma. Olympus 2T10 endoscope was passed in fasting state and the oesophagus, stomach and duodenum were fully examined. Duodenal aspirate was collected from the second part of the duodenum through a polythene tube passed via the biopsy channel. The polythene tube was specially prepared with multiple perforations on the sides. A sterile syringe was attached to the polythene tube and duodenal juice collected as described by others3. In cases where tapping was dry, 5nil. of normal saline was injected and then aspiration performed. After each endoscopy the polythene tube was first washed with plain water, then soap water and then rinse with plain water, followed by sterilization in the microwave oven for three minutes. Similarly the endoscope was cleaned with plain water, soap water and again with distilled water after each examinationAspirate (2-4 ml.) was centrifuged for two minutes and the sediment examined directly and after staining with Lugol’s Iodine. Few drops of the uncentrifuged aspirate were injected directly onto the culture media. In the middle of the study identical pathogenic organisms were obtained on several consecutive culture specimen, suggesting contamination. This was rectified by placing the endoscope in formalin vapours for five days. Cultures were retaken from the endoscope\\\'s biopsy channel and biopsy forceps. Once sterility was restored, cultures were restarted. Cultures done aerobically on blood agar and MacConkey’s media, were examined between 24-48 hours. Anaerobically thioglycolate broth was used and observations made after 48 hours. Identification was done on colony morphology, gram’s staining, reaction on TSI (triple sugar iron) and other biochemical reactions. Duodenal biopsies were also taken and examined a.fterstainingwith haemotoxylin and eosin by two different observers.
RESULTS
Ages of the patients ranged between 11-92 years with a mean age of 40.8 years. Male to female ratio was 2:1. Significant symptoms of patients harboring Giardia lamblia were epigastric pain 22.2% , dyspepsia 16.7% and diarrhoea 5.6%. Examination of the aspirate revealed Giardia lamblia in 9% (18 patients), 23% of total patients population harbored fungi. A total of 117 cultures were obtained, of which 28 got contaminated and were therefore excluded. Of the 89 cultures, growth was obtained in only 59. Candida albicans was grown on 18 cultures. Other commensals of the gut were found in small numbers too. Of the 200 patients who underwent endoscopy 36 were follow-up cases of duodenal ulcer, 6 of these had Giardia lamblia in the aspirate (33.3%). In view of the high giardia positivity in duodenal ulcer an attempt was made to determine a correlation of giardiasis with H2 receptor antagonist intake (alkaline pH favouring giardiasis). Findings obtained are given in Table.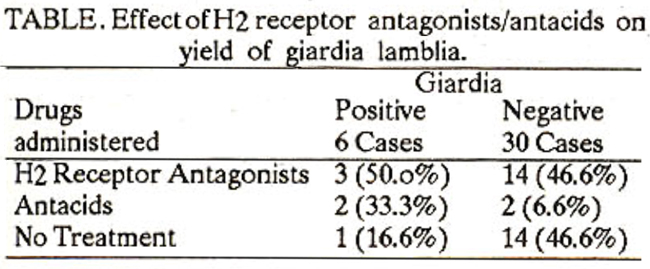
The number ofGiardialamblia positive patients was too small to reach a level of statistical significance. Atotal of 163 biopsy reports were available ofwhich 3 reported Giardia lamblia (1.8%) in duodenal tissue, 2 of these also showed Giardia lamblia on duodenal aspirate, one showed negative trohpzoites were seen in duodenal biopsy tissue.
DISCUSSION
Several methods used to diagnose giardiasi include stool examination, duodenal aspiration, mucosal impression smears and biopsy examination. The yield of Giardia lamblia in stool varied from 28.6% - 97.6%2,4-7, in duodenal aspirate from 15.5% - 64.2%2-5,8, in mucosal impression smears 57.1% - 92.3%4-6 and in biopsy specimens from 57.1% - 100%1,2,4,6,9. Giardia lamblia has been obtained in 9% of duodenal aspirates and in 1.8% of biopsy specimens in this study. Three factors which maybe responsible for the low yield include the size of the endoscopic biopsy, staining technique and excessive use of antiamoebic drugs and antibiotics in this country. Larger biopsy size was obtained with other instruments1,2,4,9 as compared to the endoscopic biopsy used in this study. Improvement of staining technique gives better results too. A 100% yield was seen with Giemsa staining9. The third factor which affected results of both duodenal aspirates and biopsy is probably the indiscriminate use of metronidazole in Pakistan. The presence of fungi, particularly Candida albicans in 18 cultures maybe due to an alkaline environment, created by 112 receptor antagonists. In those parts of the world where giardiasis is endemic, it would be best to examine 3 stool samples as suggested and then go on to duodenal aspiration, mucosal impression smears and biopsy.
REFERENCES
1. Hoakins, L.C., Winawer, S.J., Broitman, S.A., Gottlieb, L.S. and Zamcheck, N. clinical giardiaaia and intestinal malabaorption. Gastroenterology, 1967; 53:265.
2. Brandborg. L.L., Tankeraley, CS., Gottlieb, 5., Barancilt. M. and Sartor, yE. Histological demonstration of mucosal invasion by giardia IambI,., in man. Gastroenterology. 1967; 52:143.
3. Carr, M.F. Jr., Ma, J. and Green, P.H. Giardia lamblia in patients undergoing endoscopy: lack of evidence for a role in non-ulcer dyspepsia. Gastroenterology. 1988; 95: 972.
4. Kamath, KS.. and Murugasu, R. A comparative study of four methods for detecting giardia lamblia in children with diarrhoeal disease and malabsorption Gastroenterology. 1974; 66: 16.
5. Desai, HG., Kalro, RH., Zsveri, M.P. and Shreenivasan, C. Giardiaais; an evaluation of diagnostic methods. Indian 3. Gastroenterol., 1984; 3: 135.
6. Esathsm, E.J., Douglas, A.P. and Watson, A.J. Diagnosis of giardia lambli as a cause of diarrhoea. Lanceç 1976; 2: 950.
7. Wolfe, MS. current concepts in parasitology; giardiaais. N.Engl. 3. Med., 1978; 298:319.
8. Naik, SR. Diagnosis of giardiasis. Indian 3. Gaatroenterol., 1984; 3: 125.
9. Ament, ME. Diagnosis and treatment of giardisais. 3. Pediatr., 1972; 80: 633.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: