
Shahina Qureshi ( Department of Paediatrics, children’s Hospital, Islamabad. )
Naheed Qadeer ( Department of Paediatrics, children’s Hospital, Islamabad. )
Sahib Zaman ( Department of Paediatrics, children’s Hospital, Islamabad. )
Khaliq-uz-Zaman ( Department of Neurosurgery, Pakistan Institute of Medical Sciences, Islamabad. )
September 1992, Volume 42, Issue 9
Original Article
Paraplegia as a complication of malignant disease is rare in a paediatric practice. It is usually misdiagnosed as Guillian Barre Syndrome, poliomyelitis or traumatic paraplegia. Spinal cord compression due to epidural metastasis occurs in 1-4% of paediatric cancers1. This study summarizes the clinical characteristics and treatment responses of children with spinal cord compression.
PATIENTS, METHODS AND RESULTS
Of 214 children with malignant tumours admitted in the Children’s Hospital between 1987 to 1991, six (2.8%) had spinal cord compression. The diagnosis and levels of spinal cord compression were substantiated by Omnipaque myelography in all patients. Location of the lesion was confirmed by laminectomy. Biopsy and histopathology were done to confirm the tumour types. Spine roentgenography as well as examination of CSF and bone marrow were performed in all patients. The tumours presenting with spinal cord compression are shown in Table I.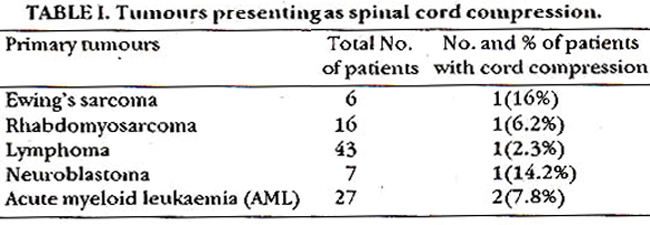
It was seen more frequently in solid tumours than in leukaemia. The clinical signs and symptoms are shown in Table II.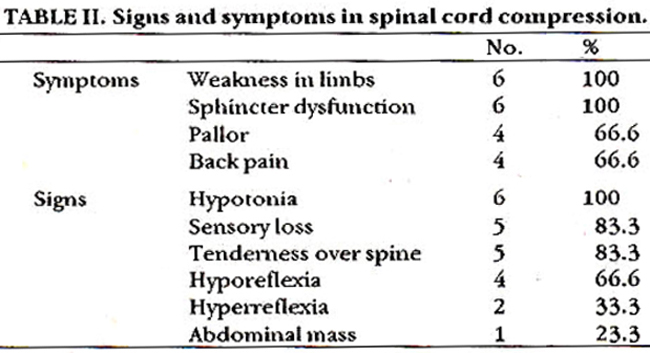
The initial symptom was back pain with gradual progression to profound weakness of the extremities in all patients. This was followed by sensory impairment in 83.3% and loss of sphincter control in 100% of cases. All patients had paraplegia at diagnosis. One patient was diagnosed as Guillian Barre Syndrome, one as poliomyelitis and one as traumatic paraplegia. Spine x-rays demonstrated bony abnormalities in 4 patients including osteolytic destructive lesions and wide disc spaces. CSF showed increased proteins in all patients. Histopathological examination of biopsy specimens confirmed solid tumours in 4 patients and leukaemia in two, which was also confirmed on bone marrow biopsy. The level of spinal cord compression in different tumours is seen in Table III.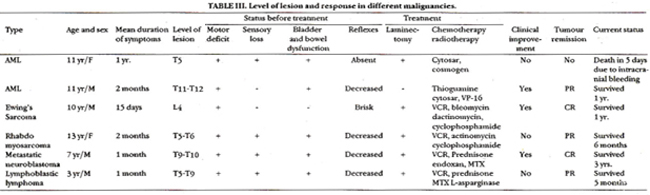
The results of treatment are also summarized in Table III. The duration of survival after spinal cord compression differed according to tumour types. All patients hadsymptoms for more than 1 week. One patient with the shortest duration of symptoms (15 days) had complete recovery of all functions and one showed improvement in muscle tone, power and bladder function. The response to treatment was negligible in patients with long durations of symptoms. Four patients survived, 2 are in complete remission one year after diagnosis. Two patients still have evidence of disease.
COMMENTS
The spinal cord and cauda equina may be compressed by a tumour in the epidural or subarachnoid space or by metastatic spread to the cord parenchyma by infiltrating through the inter vertebral foramina2. It is more frequent in solid tumours than in leukaemia1. Sarcomas account for 43-65% of metastatic spinal cord disease in children. Ewings tumour, neuroblastoma, lymphoma and leukaemia account for the rest3. Other causes are rare enterogenous intraspinal cysts and treatment related myelitis4. Congenital intraspinal neuroblastoma has been reported to cause compression in 11 patients2. Back pain which is seen in 80% of cases may be local or radicular3. Reliable localizing sign is tenderness to percussion in 80-90% of patient. There is loss of motor strength in the extremities. The progression of the clinical signs and symptoms is related to the growth rate and location of the tumour and therefore varies from one patient to another6. They may develop suddenly or progressively. Radiological abnormalities are seen in less than half of the children7. Diagnosis is confirmed by myelography. MRI has recently proved to be a useful diagnostic test7. Spinal cord compression is a medical emergency. Any plan of therapy for newly diagnosed patients should take into account the restoration or preservation of neurologic functions, the reduction of skeletal deformities and the potential for radiation induced second malignancies1. If severe or progressive, dexamethasone 1-2 mg/kg i/v is given to reduce cord edema followed by immediate myelography8. If an epidural mass is demonstrated then the spinal cord must be decompressed immediately. Both local radiotherapy and surgical decompression can be used9. Radiotherapy is given if the tumour is radiosensitive. A total of 2000 to 3000 CGY is given depending on the tumour histology6. Chemotherapy is given to patients with newly diagnosed leukaemia or lymphoma10 and started as soon as possible after diagnosis. In these patients laminectomy may not be necessary except for biopsy10. These patients have to be observed closely as an occasional child may require neuro-surgical intervention. Hayes et al have demonstrated the effect of chemotherapy alone in patients with epidural metastasis from neuroblastoma and Ewings sarcoma10.The prognosis for recovery in patients with spinal cord compression depends on the neurologic findings at the time of diagnosis1. Full recovery is possible if appropriate treatment is initiated early11.
REFERENCES
1. Lewis, D.W,, Packer, RJ., Ravey, B. etal. Incidence, presentation and outcome of spinal cord diseases in children with systemiccancer. Paediatrics, 1986;78:436-43.
2. Hrabovsky, E. and Jones, B. Congenital intraspinal neuroblastoma. Am.J.Dis. Child., 1979;133:73-75.
3. Baten, M. and Vannucci, R.C. Intraspinal metaatatic disease in childhood cancer. J.Paediatr., 1977;90:207-12.
4. Holmes, G.L., Trader, S. and Ignatiadis, F. Intraspinal enterogenous cysts. Am.J.Dis.Child., 1978;132:906-8.
5. Portenoy, iLK., Upkn, R.B. and Foley, 1CM. Back pain in the cancer patient; an alogrithm forevaluation and management. Neurology, 1987;37:134-38.
6. Allen, J.C. Management of rnetsststic epidural disease in children (editorial). J.Paediatr., 1984;104:241-42.
7. Packer, R.J., Zimmerman, R.A., Suttow, C.N. et aL MRI of spinal cord disease of childhood. Paediatrica, 1986;78:251-56.
8. Pul, C.H., Dahl, CV., Flustu, H.O. and Murphy, S.B. Epiducal spinal cord compression as the initial finding in childhood acute leukaemia and non-Hodgkin\\\'s lymphoma. J. Paediatr., 1985;106:788- 92.
9. Chien, LT., Kalwinsky, D.1C, Peterson, 0., Pratt, C.B., Murphy, S.B., Hayes, F.A.,Green, A.A. and Hustu, HO. Metastatic epidural tumour in children. Med.Paediasr. Oncol., 1982;10:455-62.
10. Hayes, F.A., Thompson, EL, Hvizdala, E., O\\\'Connor, D. and Green, A.A. Chemotherapy as an alternative to laminectomy and radiation in the management of epidural tumour.J.Paediatr., 1984;104:221-24.
11. Punt, J., Pritchard, 3., Pincots, J.R. and Till, K. Neuroblastoma; a review of 21 cases presentingwith spinal cord compression. Cancer, 1980;45;3095-101.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: