
Anjum Shahid ( PMRC Research Centre, Jinnah Postgraduate Medical Centre, Karachi. )
Anwar AIi Siddiqui ( Department of Biochemistry, Aga Khan University, Karachi. )
Sarwar J. Zuberi ( PMRC Research Centre, Jinnab Postgraduate Medical Centre, Karachi. )
Mohammed Anwar A. Waqar ( Department of Biochemistry, Aga Khan University, Karachi. )
September 1995, Volume 45, Issue 9
Original Article
Abstract
Complete absence of data on alpha 1 antitrypsin in this country prompted us to determine serum levels using radial immunodiffusion (RID) and phenotypes by isoelectric focusing (IEF) in 100 healthy adults (52 males and 48 females). Mean serum alpha 1 antitrypsin concentration in healthy subjects was 2.47±0.08 g/l and the main phenotypes MM (70%), M1 M2 (28%) and FM 3(2%) are infrequent in our population (JPMA 45:245,1995).
Introduction
Alpha 1 antitrypsin (alpha 1 AT), a glycoprotein, displays a high degree of genetic heterogeneity1 and is referred to as the protease inhibitor (PI) system. More than 70 alleles of alpha 1 AT with a variable prevalence have been identified by isoelectric focusing indifferent populations2-4. The most common form of alpha 1 AT is the MM type in most populations5 and corresponds to a normal amount of alpha I AT in serum. Other common variants include PiS. PiZ and PiF6, which are termed as deficient variants. This study was conducted to determine normal serum concentration and to identify alpha 1 AT phenotypes in the local population.
Subjects and Methods
One hundred healthy adults with no family history of peptic ulcer disease, normal liver function tests and negative endoscopy who gave prior consent to participate in the study were selected. There were 52 males and 48 females. The age range was 18-82 years (mean 33 years). Venous blood samples were drawn with minimum stasis and the clotted blood was centrifuged at 4°C. All sera were stored at -70°C until analysed. Quantitative measurement of serum alpha I AT was carried out by single radial immunodiffusion (RID) technique using M partigen immunodiffusion plates (Behring Diagnostic, Marburg, Germany7), Phenotyping was performed by ultrathin layer isoelectric focussing (IEF). Further confirmation of alpha 1 AT phenotyping was done by immunofixation8.
Results
Mean serum alpha 1 AT concentration in healthy controls was 2.47±0.08 (range 0.52-5.0 g/l). Mean values were almost similar in both sexes. The genetic variants were identified in healthy subjects by isoelectric focusing, a procedure of choice in evaluating the various phenotypes in normal population as well as in patients with diseases associated with alpha 1 AT deficiency. Atypical pattern of alpha 1 AT on IEF revealed that most of the normal individuals have a phenotype resembling MM (Figure 1).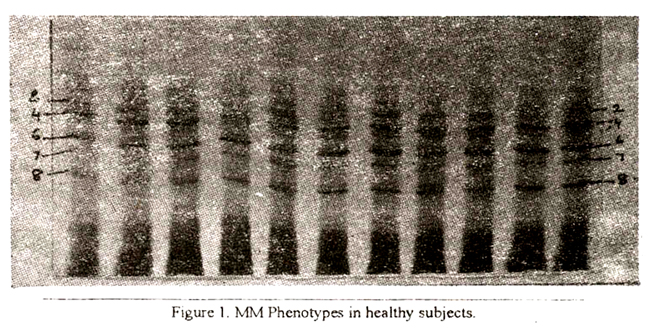
All homozygous patterns consisted of two major bands designated as 4 and 6togetherwith three minorones i.e., one anodal and two cathodal 7 and 8. - MM subtypes are presented in Figure 2.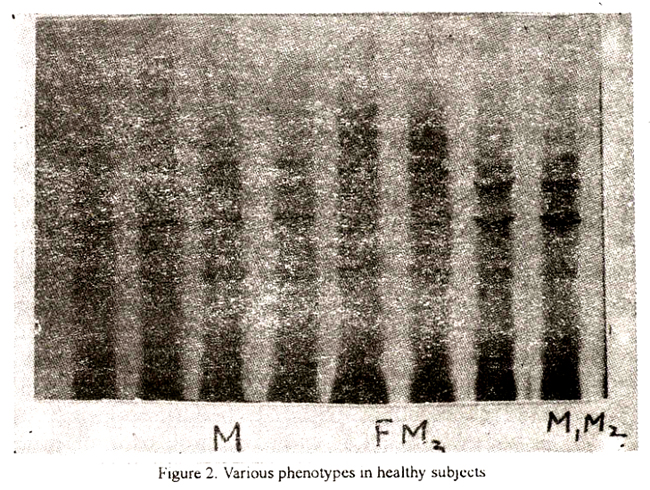
Introduction of IEF with high resolution has revealed atleast three subtypes which can be easily differentiated from one another. In the present study, MM was found in 70% of the healthy subjects followed by Ml M2(28%)andFM3 (2%):
Discussion
Normal serum levels and phenotypes of Alpha 1 antitiypsin were determined in the local population. Quantitative measurement of serum alpha 1 AT in healthy subjects shows that serum values are similar to those reported in other populations9. Since alpha 1 AT is an acute phase reactant protein, those characterized by a rapid increase in synthesis during acute inflammation8, therefore simple measurements of its blood levels may not provide the effect information regarding the status of its genetic deficiency. It is, therefore, essential to determine the phenotype of alpha 1 AT by their characteristic patterns after isoelectric focusing of serum. We, therefore, performed, isoelectric focusing analysis of each individual sample to identify the most common phenotypes among this small group of population. This study indicate that MM overwhelmingly dominates all other less common phenotypes and thus could be regarded as the normal type in Pakistan. It seems that frequency of phenotypes associated with total and intermediate deficiency of alpha 1 AT’ is substantially less in this population.
References
1. Fagerhol, M. K. and Braend, M Serum pre-albumin and polymorphism in man. Science, 1965;149:986-87.
2. Cox, D. W., Smyth. S. and Billingsley G. Three new rare variants of alpha 1 antitxypsin. Hum. Genet., 1982;61 :123-26.
3. Cox, D. W, Johnson, A. M and Fagerhol, M. K. Report of nomenclature meeting for alpha 1 antitrypsin. Hum. Genet., 1980;53:429-33.
4. Silverman, E. K., Miletich, J. P., Pierce, J. A. eta!. Alpha! antitrypsin deficiency. Am. Rev. Respir. Dis., 1989; 140:961-66.
5. Pongaew, P. and Schelp F. P Alpha 1 protease inhibitor phenotypes and serum concentrations in Thailand. Hum. Genet., 1980;54:119-24.
6. Kellermann, G. and Walter, H. Investigations on thepopulationgenetics of alpha I antitrypsin polymorphism. Hum. Gend. 1970;10:145-50.
7. Mancini, 0., Carbonara, A. 0. and Heremans, J. F. Immunochemi cal quantilica tions of antigens by single radial immunodiffusion. Immunochemistry. 1965;2:235-54.
8. Jeppson, J. 0. and Franzen, B. Typing ofgenetic variants of alpha 1 antitrypsin by isoelectric focusing. Clin. Chem., 1982;28:219-25.
9. Perlmutter, D. H. and Pierce, J. A. The alpha 1 antitrypsin gene and emphysema. Am. 3. Physiol., 1989;56:147-162.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: