
Naeem A. Zubair ( Department of Anaesthesia, Aga Khan University Hospital, Karachi. )
September 1996, Volume 46, Issue 9
Review Articles
The American College of Obstetrician and Gynecologists have classified the hypertensive disorders of pregnancy into the following four categories:
1. Pre-eclampsia or pregnancy induced hypertension (PIE) is defined as the triad of hypertension, proteinuria and generalized oedema, developing after the 20th week of gestation.
2. Chronic hypertension is the presence of sustained hypertension prior to pregnancy and continuing there into.
3. Superimposed pre-eclampsia implies the development of increased blood pressure, proteinuria, and/or oedema in a gravida with chronic hypertension.
4. Transient gestational hypertension, refers to development of hypertension without proteinuria or oederna in a previously normotensive gravida followed by return to normotension within 10 days postpartum.
Pre-eclampsia remains the most frequent, most serious and least understood of these disorders. The terminology used to define pre-eclampsia is confusing and atleast eight terntsare used in obstetric literature today1. Pre-eclampsia is a disease unique to human pregnancy;predominantly affects the young multiparas. (Frequency is 5 times higher in mothers of less than 20 years, compared to older than 20 years)2 usually occurs after the 20th week of gestation (may appear earlier in trophoblastic diseases); the prevalence is 2.5-7% of all the pregnancies in USA and accounts for atleast 20-40% maternal mortality recorded in U.S.A. and Englan3,4.
Pre-eclampsia is manifested by hypertension, proteinuria and oedema. Oedema is nota reliable sign1. Pre-eclampsia can be mild, moderate and severe. In severe pre-eclampsia, more than one of the following must exist:
1. Systolic B.P. >160 torr; DBP >110; MBP >120 ton.
2. Proteinuria in excess of 5 g/24 hours (+3->+4 by dipstick test).
3. Oliguna <500 ml/24 hours.
4. Headache, visual disturbances, cerebral disturbances.
5. Epigastnc pain.
6. HELLP syndrome (haemolysis; elevated liver enzymes; low platelets).
When grandmal convulsions occur in pre-eclampsatic patients, the syndrome is called eclampsia.
1. Pathophysiology
The cause of this multisystemic disorder is yet to be elucidated. Whether the initiating factor of this disorder is immunological, genetic or simply a decrease in uterine blood flow, is unknown. One proposed theory is immunological rejection of fetal tissues by the mother which causes placcental vasculitis and ischaemia. It appears that there are abnormalities in production and effects of circulating vasoconstricting (angiotensin and thromboxane) and vasodilating (PGE2; prostacyclin and EDRF) substances, perhaps due to widespread endothelial (immunoreactive) damage5. The abnormal changes in these hormonal levels produce generalized artenolar vasoreactivity (spasm), retention of salt and water, and altered coagulation profile (Figure).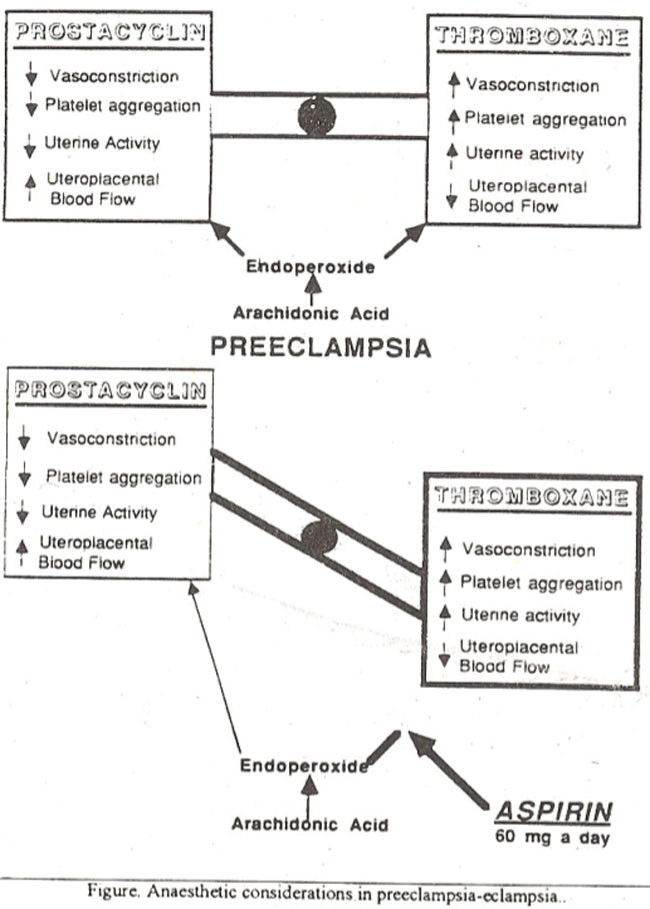
II. General management
The management is symptomatic, but the definite therapy is delivery of fetus and placenta. An early deliveiy has been stressed as crucial in avoiding serious sequelae. The main aim of management should be directed towards minimizing vasospasm, improving circulation to uterus, placenta and kidneys, improving the intravascular volume, correcting the acid base and electrolytes imbalance and above all decreasing reflex hyperactivity and central nervous system activity.
1. Bed rest: Hospitalization and bed rest in lateral decubitus position is strongly advised.
2. Hydration: Adequate hydration and intravascular volume expansion with balanced salt solution is beneficial6. Sodium intake should be adequate as salt restriction may result in increased production of renin, angiotensin and aldosterone. The use of thiazide diuretics should be discouraged7.
3. Anti convulsant therapy: Convulsions in these patients could produce deleterious effects on the mother and fetus. Commonly used anticonvulsant drugs are Benzodiazepines, Phenytoin and Magnesium Sulphate.
a. Benzodiazepines
Benzodiazepines are the first line of treatment to control convulsions in eclamptic patients. The dose for Diazepam is 5-10 mg increments until desired effects are obtained. Prophylacitically Intravenous (fly) infusion of 10 mg/hour of Diazepam can be used. Excessive sedation and airway management problems for the mother, while flaccidity, hypothermia, severe respiratory depression, low apgar score are the major disadvantages for the neonate.
b. Phenytoin
Phenytoin is gaining popularity in place of Diazepam due to lack of serious sedative side effects8. The therapeutic level is 40- 100 micro molll; which could be achieved by a loading dose of 10 mg/kg in 100 ml saline infused intravenously at a rate of 50 mg/mm (7 ml/min in a 70 kg patient), followed by a second bolus at 5 mg/kg, 2 hours later. Maintenance therapy is commenced 12 hours after the second bolus, at a rate of 200 mg/S hourly, I.V or orally.
c. Magnesium Sulphate (Mg SO4)
The agent is used for anti-convulsant and uterine vasodilatory effects. It is effective centrally and peripherally9. Magnesium Sulphate affects the neuromuscular junction by inhibiting the presy naptic calcium-facilitated transmitter release. The patients receiving MgSO4 are sensitive to Peuromuscular drugs especially non-depolarizing blockers10. The enhanced effects of Succiny lcholine is due to deficiency in plasma pseudocholinestase rather than MgSo411. Magnessium sulphate decreases peripheral resistance, increases cardiacoutput12 atemporaxy decrease in blood pressure which is offset by an increase in heart rate.
The therapeutic level is 4-6 m Eq/L which can be monitored by deep tendon reflexes and blood levels. Dose is 40-80 mg/kg followed by an infusion of 2 g/hour. In severe pre-eclampsia for the seizure prophylaxis magnesium sulphate appears to be a better choice when compared with a drug such as Phenytoin, as magnesium is an effective vasodilator even of cerebral vessels during cerebral vasospasm, while Phenytoin acts primarily by suppressing electrical activity13. In another study the best pennatal outcome was established with diphenylhydantion14.
4. Antihypertensive drugs
Commonly used drugs are Hydralazine, beta-blockers (Propranolol, Atenolol), Ca-Channel blocker (Vempamil, Nifedipine) Nitrates (Nitroglycerin), Labetalol (alpha and mainly beta blocker with predominantly beta effects), Sodium Nitroprusside.
a. Hydralazine
The primary actions of Hydralazine is to decrease precapillary arteriolar resistance. It increases cardiac output and causes reflex tachycardia. The renal blood flow is also increased. Dose is 5 mg bolus increments till the desired effects are obtained or a maximum dose of 40 mg has been administered. It is followed by a continuous IN infusion of 5-20 mg/hour(50-350 microgram/min). Maximum effect is in 20-30 minutes after I.V injection and duration is 2-3 hours. As the onset of action is slow, so repeated dosage should not be given at less than 20 minutes intervals. If sufficient time is not allowed between injections severe hypotension may ensure15.
b. Methylodopa
Methylodopa is one of the most commonly used drug in pregnancy induced hypertension. Improved fetal outcome has been reported in various studiesJt does cross from maternal to umbilical plasnta but does not cause any ill effects on the fetal heart rate patterns orfetal peripheral resistance. It is used in 1-3 G/day dosage. Over dosage will cause drowsiness, depression and postural hypotension.
c. Calcium Antagonists
1. Nifedipine 2. Verapamil
1. Nifedipine
Nifedipine is a calcium channel blocker and is effective as a safe antihypertensive agent in pregnancy particularly in Toxaemia of pregnancy16. Nifedipine causes a decrease in blood pressure. It improves uterine blood flow and fetal oxygenation17, increases renal blood flow18 and urinary output. Nifedipine is a potent uterine muscle relaxant so is useful as tocolytic agent, but could calese post-partum haernorrhage. Dosage is 10mg sublingual Nifediipin every 2 20 minutes till 30 mg is given. Also it can be used oralty. After oral administration peak effect is in 1-2 hours, witla plasma half life of 5 hours19. A combination of calcium chan blockers and MgSo4 should be used very cautiously, as hypotension respiratory difficulty and cardiac toxicity has been reported20.
2. Verapamil
When Verapamil was administered as 5-10 mg/hr via I/V infusion in patients with pregnancy induced hypertension, after fluid repletion to a pulmonary wedge pressure of 14-16 nun Hg, showed a reduction in blood pressure in a controlled manner. Both systemic and pulmonary resistance fell but cardiac output was maintained without any significant side-effects on mother and fetus21.
d. Beta-Blockers
The use of beta-blockers during pregnancy is a controversial issue. The non-selective beta-blocker are feared to be associated with increased uterine activity, decreased uterine and placental blood flow, decreased fetal heart rate and decreased fetal tolerance to hypoxia, unacceptable levels of intrauterine growth retardation and fetal mortality.
Chronic use of cardio-selective beta-blockers, such as Atenolol, appears to be effective to treat moderate to severe hypertension during pregnancy. A daily dose of 50 mg to a maximum 150 mg/day when used after 24-3 1 week of pregnancy, resulted in a better control of blood pressure with mild adverse side effects to mothers and new borns22. In anotherprospective randomized and double blind study, when Atenolol was used upto a maximum of 200 mg/day, starting from the end of the first trimester, the drug was associated with significant lower birth weight23.
c. Sodium Nitroprusside and Nitroglycerine
These drugs are to be used only in acute malignant hypertension (hypertensive emergencies). They might be useful at time of induction and intubation for a rapid control of blood pressure. Esmolol (0.5 mg/kg bolus followed by 0.3 mg/kg/min) or Labetalol 5 mg incremental bolus dosages till 1-2 mg/kg also have been administered with success mainly at induction and intubation times24.
III. Anaesthetic considerations
One should keep in mind the following points while assessing/managing a patient inlaborwith severe pre-eclampsia.
1. Cardiovascular systems
There is reduced circulating blood volume with haemoconcentration which will mask the presence of anaemia. The volume depletion may lead to an exaggeration of the response to aortocaval compression, therefore, left uterine displacement must be employed. Intravenous fluid loading under the continuous monitoring of CVP or pulmonary capillary wedge pressure and urine output is necessary before the conduction of regional or general anaesthesia. There is still controversy about the type of fluids (crystalloid versus colloid) for preloading and replacement. Volume loading should be done with caution as these patients have leaking capillaries, decreased oncotic pressures25 and reduced ventricular compliance. Nisell et al26 examined the effects of acute plasma volume expansion on atrial nathuretic peplide concentration in 16 pre-eclamptic patients and compared with 16 healthy control patients. Atrial natriuretic peptide (ANP) has diuretic smooth muscle relaxing and hypotensive properties and is known to reduce blood volume by increasing capillary permeability. As a result of volume load this peptide is secreted. There is an enhanced response to ANP in preeclamptic patients, also there is an increased level in preeclamptic patients. AMP is slowiy cleared owing to poor renal function and endothelial damage. The increased level of ANP may further exacerbate the capillary leak enhanced fluid loss and protein into extravascular space. The data strongly suggests against raising the right atrial pressure to “normal levels”. Woods et al27 found a six-fold increase in incidence of CCF and four-fold increase of acute respiratory distress syndrome within 24 hours postoperatively in the pre-eclamptic patients as a result of over enthusiastic fluid loading. Rapid infusion of crystalloid fluid may significantly lower the colloid oncotic pressure for 24 hours28, which may not be tolerated by these patients and end up in pulmonary ocdema29. 500-1000 ml of 5% Albumin in severe pre- eclamptics increases cardiac output, decreases systemic vascular resistance with no or minimal effects on the mean arterial blood pressure30. The colloidal solution (plasma protein fraction or Albumin 5%) seems to be a preferable choice in severe preeclamptic patients. Both fluid regimes have their proponents and opponents. Crystalloid fluids should be without Dextrose. A balanced crystalloid solution or 0.9% Nacl solution upto a volume load of 500 ml-l000 ml is well tolerated in these patients with epidural analgesia upto T10 level. A combination of colloid/crystalloid could be a better choice in these patients.
2. Laryngeal oedcma
Retention of sodium and waterand exaggerate effects of normal pregnancy hormones lead to the development of laryngeal oedema in pre-eclamptic patient. This could cause intubation and post- operative ainvay management difficulties.
3. Coagulopathy
In the severe pre-eclamptic/eclamptic patients, coagulation disorder might be markedly present. At admission it is necessary to obtain a complete blood picture with platelets count, followed by serial platelet counts when monitoring intra-partum coagulation indices. Evaluation of PT, PTT and flbrinogcn to be added only if platelet count is less than 100.000 per mm331. A rapid change in platelets count is a more significant event rather than an absolute value32. Platelet functions, rather than number is more important33, but tests (Thromboelastography) to check the function are time consuming and expensive. About 10 to 25% of pre-eclamptic patients with normal platelet counts have prolonged bleeding time33,34.
Schindler et al34 recommended that bleeding times should be performed on all patients with platelet count between 50,000- 100,000/mm3 prior to invasive regional techniques but some feel that bleeding time is not a good indicator for coagulation disorders. Fibrin D-Dimer analysis has been proposed as a more sensitive and early indicator on intravascular coagulation and fibrinolysis than standard coagu lation tests35. Only if significant coagulation disorderexist with a platelet count falling under 100,000 mm3. a prolonged bleeding time or an abnormal TEG (Thromboelastography) then regional anaesthesia is relatively contraindicated36
Epidural is absolutely contraindicated when platelets are less than 50,000 mm3. While when platelets are between 50,000 to 1,00,000 per mm3 risk benefit balance should be assessed as possibility toepidural haematoma incidence is 1:10,000 cases. There are yet no clear guidelines foracceptable safe limits but a level of platelets >100,000 mm3 or a bleeding time of<10 minutes is commonly used37. In the presence of coagulopathy
significant bleeding can occur during laryngoscopy for oral intubation. Attempts should be very gentle and careful.
4. Drugs interactions
There could be significant effects on the mother’s cardiovascular, muscular, CNS and other systems, due to the interactions between therapeutic drugs and anaesthetic drugs/techniques.
a. Magnesium sulphate and muscle relaxants
The interactions between magnesium sulphate and muscle relaxants is well documented. The reduction in the dosage and a continuous monitoring of neuromuscular function with the help of peripheral nerve stimulator is advisable. b. Magnesium sulphate and regional anaesthesia
The neuromuscular weakness and potential hypotensive effects of magnesium sulphate might be slightly exaggerated with sympathetic blockade, but the protective and beneficial effects on the uterine and umbilical blood flow due to epidural anaesthesia eliminates the increased fetal risk21, so combination is assumed to be safe. Subarachnoid block for higher level is not widely recommended due to rapid onset of sympathetic block and risk of severe hypotension38,39
c. Use of low dose aspirin and epidurals
The use of low dose aspirin (60 mg/day after the 12th week of pregnancy is based on the rationale that at this dosage aspirin produced an inhibition of lipid peroxide and thromboxane production but not prostacyclin production, thus protecting against both vasoconstnction and pathological clotting). Concerns have been expressed about placing epidurals in patients receiving aspirin as their antiplatelet actions might increase risk of epidural haematoma. A large multicentral40 randomized placebo control trial to evaluate the effects of low dose aspirin to prevent and treat pre-eclampsia failed to show any significant adverse effects on coagulation profile of these patients. There is also no data to recommend routine bleeding tests on these patients as bleeding time does into indicate the risk of bleeding. Orlikowsk et al41 noted that chronic use of low dose of Aspirin does not seem to be associated with TEG (Thromboelastography) changes.
5. Antihypertcnsive drugs and anaesthetic drugs When anaesthetic drugs are administered to the patients who are on antihypertensive treatment cardiovascular depression may be more pronounced and marked. The careful choice of anaesthetic drugs and dosage is mandatory. There is a need for titration of the dose of anaesthetic drugs.
IV. Hyperexaggerated Response
There is increased vascular reactivity which results man intensified response such as tachvcardia, severe hypertension, due to the release of catecholamines. This particular problem is apparent during with laryngoscopy, in light general anaesthesia and at extubation. Such sudden rises in blood pressure may increase the risk of cerebral haemorrhage and oedema, myocardial infarction, pulmonary oedema or cardiac failure39. Techniques and drugs should be used to obtain or completely abolish these responses. The general recommendations are to use drugs such as short and rapidly acting anti hypertensives, xylocaine intravenously or high doses of narcotics, before induction and laryngoscopy.
The stress responses to laryngoscopy could be obtunded by nitroprusside 0.1 to 3 micrograms/kg/min, just prior to induction42. Labetalol 20 mg given intravenously foliwed by 10 mg increments to a total dose of 1 mg/kg resulted, in reduction in mean artery blood pressure and heart rate and the cardiovascular response to laiyngoscopy and intubation were reduced.
Nitroglycerine 0.1 micrograms/kg/min was not effective in preventing the hypertensive responses to laryngoscopy while Esomolol could prevent the hypertensive response but has caused fetal hypoxemia in animal studies43. Fentanyl I micrograms/kg or Alfantanil 10 micrograms/kg given at induction attenuated these responses but did not abolish them completely44.
V. Pre-anaesthetic management/monitoring
Before any procedure is undertaken, it is mandatory to optimize the condition of the patient. We should try to control the blood pressure, restore blood volume, improve renal function, institute anticonvulsant therapy (if indicated) and initiate proper monitoring. The minimal monitoring employed should be blood pressure by a non-invasive method, heart rate and urine output measurements. Direct intra-arterial blood pressure monitoring is indicated in patients with severe pre-eclampsia or eclampsia.
Central venous pressure monitoring is indicated in severe pre- eclamptic and eclamptic patients as a minimal invasive monitoring. They have clearly reduced blood volume and are fluid deficient. Volume loading is often necessary, which could cause pulmonary oedema. Some anaesthesiologists recommended the use of pulmonary arter catheter (P.A.C) for effective management of patients. Informations gathered from P.A.C. can be used to institute therapy such as fluid challenges, potent vasodilator infusion and beta adzcnergic blockade to optimize the patients haemodynamic status45. P.A.C. is also indicated in pre- eclarnptic/eclampsia patients with unresponsive oliguria, pulmonary oedema and in those cases where epidural anaesthesia is contemplated. However, some workers do not think that pulmonary catheterization is strongly indicated and useful46. Electronic monitoring of fetal heart rate and uterine contractions is essential, when labour is artificially induced or epidural analgesia is instituted. Fetal blood analysis for PH may be indicated when significant fetal heart rate abnormalities occur.
VI. Choice of Analgesia
Choice of analgesia will depend on obstetrical situation, the status of the patient and the condition of the fetus (if still in utero). Narcotics provide good analgesia but have no anticonvulsant and antihypertensive properties. Tranquilizers in combination with narcotics are in use and have variable success with significant side effects. Patient controlled analgesia (PCA) with Fentanyl (loading dose of 50-100 micrograms followed by 25-50 micrograms hourly) or Meperidine (25-50 mg followed by 10-15 mg/hour) may be used. A mixture of N20 and ox-ygen(50:50%) provides good analgesia and increases oxygenation. This combination is effective during the late first stage and at delivery time. Addition of 0.5-0.75% Enflurane or 0.3-0.5% Isoflurane or 0.5% Halothane to N20 plus 02 admixture could produce the effective desired results for delivery. Local infiltration of perineum or Pudendal nerve block provides satisfactory analgesia for most forceps deliveries.
Epidural analgesia
The use of continuous lumbar epidural analgesia in severe pre- eclamptics/eclamptics whose convulsions are under control is widely accepted and recommended45,47-49 unless contraindicated due to gross coagulation abnormalities, or marked untreated hype- volumia, or maternal septicemia. Properly conducted epidural analgesia for labourand delivery, decreases maternal oxygen requirenients, prevents maternal hyperventilation, significantly decreases circulating levels of Epinephrine50: increases intervillous blood flow51; appears to protect against eclamptic convulsions52; chances of pulmonary aspiration are minimized and stabilizes the blood pressure at modestly lower levels. All these effects cause an improvement in mother’s clinical status; moral attitude and fetal well being. Apgar score in neonates born to mothers with Epidural was far better than non-epidural group. Concerns expressed by others are that epidural analgesia should not be used in severe pre-eclamptic patients53. Sudden hypotension which could be deleterious to already compromised fetus due to further decreases in uteroplacental blood flow54. Also anaesthetics used could decrease fetal beat-to-beat variability and impede the diagnosis of fetal hypoxia and distress55. Due to cOagulopathy, in pre-cclamptic patients formation of epidural haematoma is a possibility during invasive regional techniques.
Studies have shown that. properly conducted epidural analgesia/anaesthesia does not cause significant hypotension or fetal distress56. The decrease in blood pressure is comparable with non pre-eclamptic normal patients57,58. A sequential technique, of raising the block in stages. rather than in a bolus is the generally favoured approach. Ephedrine is the drug of choice for hypotension59. Animal and human studies, including studies in pre-eclamptic parturients showed that intervillous blood flow was maintained or improved with the use of epidural analgesia61,60. Anecdotal reports of epidural or subarachnoid block inadvently administered to patients with platelets counts <100,000 mm3 have not described any epidural haernatorna as a consequence61. Epidural block administered before delivery in pre-eclamptic patients have not resulted in epidural haematoma even if the platelet numbers have decreased below 50,000 mm3 after delivery. It is advisable to leave the catheter in place till the coagulation profile including platelets are within normal acceptable limits.
The use of adrenaline in epidural space is controversial. Administration of adrenaline mixed local anaesthetic could cause severe hypertensive response in patients with preeclampsia/eclampsia, due to increased sensitivity to catecho lamine. However, others62 think adrenaline is safe as only B-adrenergic effects are seen. Lidocaine does cause a slight decrease in fetal heart beat to beat variability, while Bupivacinc use is not associated with decrease in fetal beat to beat variability63. Ideally, in patients with severe pre- eclampsia institution of epidural analgesia should be proceeded by placing a CVP or Pulmonary Artery Catheter64. Such patients should receive a balance salt solution and/orcolloid until CVP is +3/+4 ems of water or pulmonary capillary wedge pressure is 5- 12 mmHg65.
In view of the vast favourable clinical experience and recent investigational work, the evidence supports the use of epidural analgesia for labor, vaginal delivery and Cesarean section in most mothers with severe pre-eclampsia or controlled eclarnpsia59.
General anaesthesia
While planning for general anaesthesia, the hazards and possible pmblems which could be encountered in severe pre-cclamptic patients should be kept in mind. The major hazards are difficulties in airway maintenance, excessive and aggregated response to laiyngoscopy and endotracheal intubation. interaction of anaesthetic drugs with drugs used by obstetrician particularly magnesium sulphate. Despite various hazards, some authorities feel that risks of rneral anaesthesia are less than those of regional anaesthesia66 while others feel that general anaesthesia has markedly increased risks67.
Operation of the patient for general anaesthesia
a) P re-induction period
The earlier involvement of the anaesthesiologist is very important. The clinical condition of the patient should be optimized before surgery. Blood pressure and convulsions should be properly controlled. All antihypertensive and anticonvulsant drugs to be continued till patient is in the operating room. It is advisable to bring patient to the operating room in the lateral position and have oxygen via face mask during transportation. The usual doses of antiemetics (Metocloprarnide 10 rug IM) and antacids (Sodium Citrate 0.30 mmol, 30 ml) or a H2 histamine receptor antagonist (Ranitidinc or Cimetidine or Famotidine) be given orally 1-2 hours prior or 40-60 minutes earlier intravenously.
b) Induction period
In case of severe fetal distress or compromise, intravenous induction with agents such as Thiopentone sodium or Propofol is likely to reduce placental perfusion with further detrimental effects to the fetus. Ketamine is contraindicated while Etomidate has been condemned for undesirable effects on adrenocortical axis, but is a relatively cardio stable drug. There may be ajustification for the use ofbenzodiazepines for induction especially, when a specific benzodiazepine receptor antagonist (Flumazenil) is available. The exaggerated pressor responses to laryngoscopy and intubation could be attenuated by various techniques using drugs such a Hydralazine, Labetalol or Sodium Nitroprusside. A rapid sequence technique should be used to secure the airway.
Intra-operative l)CflOd
Institution of LPPV can adversely affect the uterine blood flow by reducing cardiac output especially in dehydrated or volume depleted patients. These patients should be kept normocapnic or somewhat hypcrcapnic to improved placental blood flow and decrease shunting. Hyperventilation should be avoided as it will lead to deterioration in uterine/placental blood flow due to decrease in cardiac out-put, vasoconstnction and respiratory alkalosis which will shift the oxygen dissociation curve to the left.
It is well known that Nitrous Oxide has low lipid solubility and it has relatively rapid transplacental passage which can cause some degree of neonatal depression during C-section. There is probably a slight but definite real risk that the already hypoxic infant may be adversely affected by this agent. However, if an unacceptable risk of maternal awareness at operation is to be avoided due to low nitrous-oxide concentration or no nitrous oxide imposed by a high FIo2, additional vapor (inhalational) supplementation will be required. In general the available evidence suggest that Halothane in a concentration of 1.0 MAC or less has little or no effect on placental perfusion or fetal well-being, while higher concentration result in deterioration68.
Various studies50,69 failed to show any adverse effects due to Halothane or Enflurane on the fetus as determined by neonatal apgar score, acid-base status or earlier neuro-behavioral score when compared with the other group which reccivedoxygen/nitrous oxide maintenance. Also 0.5%orless Halothane is not associated with increased blood loss. Enflurane in low concentration is devoid of any adverse effects on neonates when used as a supplementary agent in subanaesthetic concentrations during labour50,69 Isoflurane has gained popularity due to properties of low blood solubility, apparent freedom from hepatic and renal toxicity and relative cardiovascular stability. At equipotent concentrations it’s effects on uterine contractility is similar to Halothane and Enflurane70, while maintaining normal maternal and neonatal conditions. In another study, Isoflurane 0.75%was found to be preferable to 0.5% halothane during cesarean section because of more rapid recovery, less bleeding and less uterine relaxation. Intra-operative muscle relaxation could be maintained by Suxamethonium infusion (4 mg/min or small boluses of a depolarizing agent in incremental doses, e.g., Vecuronium (1-2 mg) or Atracrium (10-15 mg) adjusted as necessary using a nerve stimulator.
Extubation
The cardiovascular changes due to extubation could be as severe as pressor responses to intubation. At this moment, neither narcotics due to their respiratory depressant effects nor Magnesium Sulphate due to its neuromuscular blocking properties are likely to be ideal. The idea of extubating these patients in the deeper planes should be addressed very carefully due to high potential for airway management difficulties and aspiration. There is sonic role for vasodilators or beta-blockers especially short acting such as Esmalol at this stage.
Post-operative care
The delivery of the fetus and placenta is the treatment but the full recovery may take 10 days to 2 weeks. The airway management may be more difficult in the postoperative period due to the worsened laryngeal oedema situation. Respiratory embarrassment may be severe and airway maintenance may be impossible without anendotrachealtube. The antihypertensive and anticonvulsant drugs should be continued in the postoperative period as long as indicated. It is very important to keep these patients pain free with good analgesia. Epidural analgesia is an ideal choice, if epidural catheter is in place. These patients should be closely and maximally nionitored (both invasively and non-invasively) in the Intensive Care Unit at least for the first 24 hours.
Key points for anaesthetic considerations
1) Essential monitoring:
a. Non-invasive monitoring. e.g.. ECG. pulse rate, blood pressure, pulse oximetrv. urine output.
b. Invasive monitoring, e.g., CVP. Swan Ganz Catheter, intraarterial blood pressure.
2) Prevention and control of convulsions by use ofMagncsium Sulphate, Diazepam and Phenytoin.
3) Optimal stabilization of cardiovascular system by careful fluid balance and use of vasodilators.
4) Proper pre-anaesthetic evaluation of various systems with specific attention towards cardiovascular, renal coagulation and hepatic system.
5) Anaesthetic choices:
a. Regional anaesthesia
A carefully administered epidural blockade is strongly advised, unless gross contraindications exists. Epidural is absolutely contraindicated when platelets are less than 50,000/mm3. while between 50.000-100,000/mm3, the risk balance should be assessed as possibility of haematoma incidence is 1:10,000 cases.
Subarachnoid block is not widely recommended due to the risk of sudden and severe hypotension.
b. General anaesthesia
It requires skilled ainvay management. control of pressor response to laryngoscopv and intubation, awareness of the potential drugs interactions and careful postoperative management.
6) Avoidance of certain drugs i.e.. Methoxyflurane, Ketamine and Methergin: reduction in dosage of Vasopressors when needed; prophylactic use of Ephedrine is not recommended and titration of muscle relaxant drugs.
7) Proper management in the I.C.U. in the postoperative period. Anticonvulsant and antihypertensive drugs to be continued as indicated. Good analgesia could be provided via the epidural route.
8) The successful management of these patients depends upon the team work and communications of obstetrician, mid-wife and anaesthcsiologisL all of whom have iniportant roles to play. While (lie majority of patients require minimal intervention, severe pre-ectamptic patients need expert care with excess to invasive monitoring and therapy in the intensive care units.
References
1. Sibat, B M Pitfalls in diagnosis and management ofprc. eclampsia (Editorial) Am J Obstet Gynecol., 1988;159:1
2. SaflIas, A.F. Olson, I) R.. Franks. A.. ct at Epidemiology of pre-eclampsia and cclampsia in thc United States, 1979-1986 Am. J. Obstet. Gynecol.. 1990; 163:460-465.
3. Atrash. IlK . Kodninc, L M.. 1.awson, H %V et at. Maternal mortality in the United Statcs. 1979.1986 Obstet. Gynecol.. 1 990;76: 1055.1060.
4. I lood. DD Maternal and Fetal Morbidity and mortality. Ch. in James FM Wheeler, A S and Dewan. D. (eds). Obstetric anaesthesia The complicated patient. 2nd edition. Philadelphia. FA Davis. 1988. pp. 58-59.
5. Lockwood, C.J and Peters. J H. Increased levels of EDI cellular fibronectin proceed the clinical signs of preeclampsia Am. J. Obstet. Oynae. 1990.162 358-362
6. Kirskon, B., Motec. K J . Cotton. D. B et at Role ofvolume expansion in severe prceclampsia. Surg Gynecol Obstet., 1988,167.367-371.
7. Davidson, J.M. and Lindhermer. M.D. Hypertension in pregnancy In Disease of the Kidney. 4th ed Schrier. R \\\\V and C. Gottschalk. C.tV. eds. Boston Little Brown, l988.pp 1653.1688.
8. Ryan. 0 . Lange, I R and Naugler. MA. Clinical experience with phcnytoin prophylaxis in severe preeclampsia Am. J Obstet Gynecol.. 1989.161:12971304
9. Pritchard, J.A. The use of magnesium sulfate in preeclampsia. J. Reprod. Med., 1979.23. 107.
10. Skaredoff. MN. Road, E.R and Datta, S. Hypermagncsemia and anesthetic management Can J Anaesth . 1982;29:35-41
11. Kambarn. J. R.. Perry, SM. Entman. S et al. Effects of magnesium on plasma cholinesterase activity Am J. Obstet Gynecol.. 1988; 159:309-311.
12. James. M. F.M.. Cork, R.C. and Dennett. J E. The effect of magnesium sulphate on the cardiovascular system of the baboon. Magnesium, 198 7;6: 314-324
13. Belfort, M.A. and Moioce, K J Effects of magnesium sulphate on maternal brain blood flow in pre-eclampsia A randomized placebo controlled study Am, Obstet Gynecol . 1992;167:661-666
14. Maheshwari J.R . Deser. S V and Hansotiamd-Walvekar, yR. Anticonvulsant therapy in eclampsia J. Postgrad.Med., 1989;35:66-69
15. Naden, R.P. and Redman. C W.G. Antihypertension drugs in pregnancy Clm Perinatal , 1985.12 521-525
16. Luric. S.. Fenaket. K. and Friedman. A. The effects of Nifedipine on fetal heart rate in the treatment of severe P.lH. Am J. Perinatal., 1990;7:285-6.
17. Norris, MC.. Rise., J C and Dewan, D.M. Nifedipine orverapamil counteracts hypertension in gravid ewes Anesthesiology I 986;65 :254-58.
18. Barton. JR.. Hiett AK. and Conover, W.B. The use of nifedipine during the postpartum period in patients with severe preeclampsia. Am. J. Obstet Gynecol., 1990.162:788.792,
19. Fox, E.J., Sklar. G.C.. Hill. C.H. et at. Complications related to the pressor response to endotracheal intubation. Anesthesiology, 1 977;47: 524.525.
20. Vijay. CS. and David, J.T Ch. calcium channel blocker, Modern pharmacology. (Edt) Craig. R.C and Sutzel. E.R 4th edition. New York. Little Brown and Company. 1994. pp. 249.254
21. Belfort, M A . Anthony. J.. Buccimazza. A. et al Hemodynamuc changes associated with iv infusion of verapamil. Obstet. Gynecol., I 990;75:970.974
22. Fabreques. G , Alvarez I . Juri, P.V et al. Effectiveness ofatenolol in treatment of hypertension during pregnancy Hypertension. 1992,19 (Suppl) 129-131
23. Butters, L.. Kennedy. S and Rubin. PC. Atenolol in essential hypertension during pregnancy Br Med J., 1990,301:587.589
24. Eisenach, J.C. Mandell. G. and Dewan, D.M. Materual and fetal effects of labetalol in pregnant ewes Anesthesiology, 199134:292-297
25. Drown, M A Pregnancy induced hypertension. Current Concepts Anaesth Intens Care. 1989,1 7185-197.
26. Nisell H , Carlstrom K , Cizmsky S. et al. Atrial natriuretric peptide contractions and haernodynamic effects of acute plasma volume expansion in normal pregnancy and preeclampsia. Obstet Gynecol., 1 992;79:902-907.
27. Woods, J.B., Blake, PG. Perry, KG Ascites, a portent of cardiopulmonary complications in preeclamptic patient with the syndrome of haemolysis. elevated liver enzymes and low platelets. Obstet. Gynecol. 1992;80:87-9 I
28. Jones, MM. Longmire. S.. Cotton. D.B. et at Influence of crystalloid versus colloid infusion on periparlum colloid osmotic pressure changes. Obstet, Gvnecol , 1986.66659-661.
29. Benditti. T.J, Kates, R. and Williams, V. Hemodynamic observations in severe preeclampsia complicated by pulmonary edema. Am. .1. Obstet Gynecol., 1985:152:330-334.
30. Wasserstrum. N., Kirshon, B., Willis, R.S. et al. Quantitative hemodynamic effects of acute volume expansion in severe precclampsia. Obstet Gynecol., 1989;73 .545-550.
31. Leduce, L, Wheeler, J.M., Kirshon, B. et al Coagulation profile in severe preeclampsia. Obstet. Gynecol. 1992;79: 14-18.
32. Davis, H C. Anaesthesia for high risk obstetric patients 44th Annual Refresher Course Lectures and clinical update program Washington D.C., USA. ASA Inc, 1993,412,pp. 1-7.
33. Kelton, J.G - Hunter, D.J S and Nesame, PB A platelet function defect in prceclampsia Obstet (ivnecol, 1985;65 107-109.
34. Schindler, M , Gait, S. Isert, P. et al Thrombocytopenia and platelet functional defects in preeclampsia, Implications for regional anaesthesia. Anaesthesia and Intensive Care, 1990;18:169-174.
35. Trofatter, K E - I lowell, M L., Greenberg. C. S et al. Use of the tibrin D-dimer in screening for coagulation abnormalities in precclampsia Obstet Gynecol., 1989.73(3)435-439
36. Andrew, M Malinow: Precclampsia and elampsia Anaesthetic management. 44th Annual Refresher Course Lectures and Clinical update Program. Washington, D.C , ASA Inc. Washington. D.C. . USA. 1993,235 pp.1-7.
37. Howell, PR and Rubin, A.P Pre.eclampsia. eclampsia and the anaesthetist. Curr. Anaesth. Crit Care, 1991;20:101-107
38. Mudie, L.L. and Lewis, M Pre-ecalmpsia Its anaesthetic implications Br J. Hosp. Med., 1990;43:297-300.
39. Ramanathan, S. and Sobao B.M. Obstetric anaesthesia 2nd edition,(Edt) Philadelphia. Ramanathan S Lea and Febiger. 1988; 151-166.
40. De Swiet-Redman, C.W.G. Aspirin, Extradural anaesthesia and the MRC collaborative low dose aspirin study in pregnancy. CLASP (Letter) Br J. Anaesth., 1992;69:109-110.
41. Orlikowski, C.E.P.. Moodley, 7. and Rocke, D.A. Thromboelastography in pregnant patients on low dose aspirin (letter). Lancet, 1992,338 1267-1277.
42. Stoelting. R K. Attenuation of blood pressure response to laryngoscopy and tracheal intuhation with sodium Nitroprussude. Anaesth Analg (Cleve), 1979;58:116-119.
43. Eisenbach, J.C. and Castro, M. I Maternally administered esmolol products fetal adrenergic blockade and hypoxemia in sheep. Anesthesiology. 1989,71:718-722.
44. Darm, W.L., Hutchinson, A and Cartwright, D P Maternal and neonatal responses to alfentanil administration before induction of general anaesthesia for caesarean section.Br. J. Anaesth., 1987;59:1392-1396.
45. Clark, S.L. and Cotton, D.B. Clinical indications for pulmonary artery catheterization in the patient with severe precclampsia Am. 7. Obstet Gynecol., 1988;158:453-458.
46. Cunningham. F.G. and Lindheimer, M D Hypertension in pregnancy N Engl. 7 Med., 1992;326:927-932.
47. Hibbard, B NI and Rosen, NI. lhe management in severe pre- eclampsia and cclampsia. Br. 7. Anaesth., 1977;49:3-9.
48. Moir, D.D., victor-Rodriques, L and Willocks, J. Extradural analgesia during labour in patients with pre-eclampsia J. Obstet. Gvnaecol Br. Commonw., 1972;79:465-469.
49. Gutsche, B.B. The experts opine; The role of epidural anaesthesia in precclampsia Surv. Anesthesiol., 1989:30:304-311.
50. Abboud, T., Anal, R , Sarkis, F et al. Sympathoadrenal activity, maternal, fetal and neonatal responses after epidural anaesthesia in the preeclamptic patient. Am. J. Obstct. Gynecol., 1982;144:91: 5-918.
51. Jouppila, P.. Jouppila. R.. Hollmen A. et al. Lumbar epidural analgesia to improve intervillour blood flow during labor in severe precclampsia Obstet. Gynecol., 1982;59 158-161.
52. McneIl, D.A., and Koch. M.A.T Epidural anesthesia as an anticonvulsant in the management of hypertensive and eclamptic patients in labour S Air Med J., 1980;58:875-877.
53. Pritchard, 7 A., Cunningham. F G. and Prichard, S. A ilie Parikland Memorial Hospital protocol for the treatment of eclampsia-evaluation of 245 cases Am. Obstet. Gynecol .1984;148:951-963.
54. lion E.H., . Reid. B L and Hehre, FW The electronic evaluation of fetal heart rate. II Changes with maternal hypotension. Am J Obstet. Gynecol., 1960;79:209-215.
55. Boehm, F., Woodruff. L and Growdon. J. The effects of lumbar epidural analgesia on the fetal heart rate baseline variability Ancsth. Analg., 1975;54:779-782.
56. Moore, T R., Key, T C, Reisner, L.S. ci al. Evaluation of use of continuous lumbar epidural anesthesia for hypertensive pregnant women in labor. Am. J. Obst. Gynecol., 1985;152 404-412.
57. Kaar, K., Joupplila, P.Kuikka, J et al Intervillous blood flow in normal and complicated late pregnancy measured by means of an intravenous Xe method. Acta. Obstet. Gynecol Scand, 1980.59 7-10.
58. Lopcz-Liera, M Complicated eclampsia Fifteen years experience in a referral medical center. Am 7 Obstet Gynecol., 1982,142:28-35.
59. Cotton, D.B., Lee. W, Huhta. J.C et al Hemodynamic profile of severe pregnancy-induced hypertension Am J Obstet. Gynecol., , 1988,158:523-529.
60. Jouppila, R. Jouppila. P.. Hollmen, A. et al Epidural analgesia and placental blood flow during labour in pregnancies complicated by hypertension Br. J Obstet. Gynaecol. 1979,86:969-972.
61. Rasmus, K.T., Rottman, R L . Kotelko, D.M et al Unrecognized thromboeytopenia and regional anaesthesia in parturients. A retrospective review. Obstet Gyneeol.. 1989.73:943.946.
62. Heller, P.7. and Goodman. C. Use of local anesthetic with epinephrine for epidural anesthesia in preeclampsia. Anesthesiology, 1986;65:224-226.
63. Lavin, J.P. The effects of epidural anesthesia on electronic fetal heart rate monitoring. Clin Pcnnatol. 1982;9:55-62.
64. Strauss, R.G., Keefer, J R. Burke. T ci al. Haemodynamic monitoring of cardiogenenic pulmonary edema complicating toxemia of pregnancy Obstet Gynecol., 1980;55:170-1 74.
65. Joyce, T.H., Debnat K.S. and Baker, E. A. Preeelampsia relationship ofCVP and epidural analgesia. Anaesthesiology 1979;51 :S297.
66. Altura, B.T. and Altura, B Ni. Interaction of Mg and K on cerebral vessels. Aspects in view of suoke Review of present status and new findings Magnesium, 1984;3:195-211.
67. Crowhurst, J.A General anaesthesia in obstetrics, Curr. Opin. Anaesthesiology. 1911;3: 349-355.
68. Eng. M, Bonica. W.J Akarnasu, T et al. Maternal and fetal responses to halothane in pregnant monkeys Acts Anaesthesol. Seand., 1975;19:154-156.
69. Abbound, T.K., Kin, S.H., Henriksen, E. et al. Comparative maternal and neonatal effects of halothane and enflurane for caescrean section. Acta Anesthesol Scand, 1955;29:663-668.
70. Munson, ES. and Embro, W.J. Enflurane. Isoflurome and halothanc and isolated human uterine muscle Anaesthesiology, 1977;46: 11-14.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: