
Shumaila Zia ( Department of Gynaecology/Obstetrics, College of Medicine King Khalid University, Abha, KSA. )
Muhammad Rafique ( Department of Paediatrics, College of Medicine King Khalid University, Abha, KSA. )
June 2013, Volume 63, Issue 6
Original Article
Abstract
Objective: To compare the pregnancy and neonatal outcome in sickle cell disease and trait women.
Method: The retrospective comparative study was conducted at Abha General Hospital, Abha, Saudi Arabia, from January 2009 to December 2011. The records of women having sickle cell disease and trait were reviewed for antenatal and postnatal complications. Pregnancy and foetal outcome was also compared in both the groups. Chi-square, Fisher\\\'s Exact and Student\\\'s t tests were used for statistical analysis.
Results: Out of 112 women, 57 (50.89%) had sickle cell disease and 55 (40.10%) had sickle cell trait. The mean gravidity and parity in the latter group (5.05±3.51 and 3.2±2.74 respectively) was more than double in the former group (2.89±1.36 and 1.66±0.96 respectively). There were significant differences in antenatal complications. In the disease group, anaemia was in 55 (96.5%) cases compared to 35 (63.6%) in the trait group. Significant number of women in the first group (n=41; 71.9%) experienced painful crisis in pregnancy compared to 4 (7.27 %) in the second group. Mean haemoglobin in the disease group was 8.35g/dl, while it was 9.96 g/dl in the other (p <0.01). The requirement of blood transfusion was higher in the former, 28 (38.6%) than in the latter 3 (5.54%). Frequency of pre-term delivery was only slightly higher in the disease group, 14 (28.57%) than in the trait women, 13(23.63%). The mean birth weight of babies of women with the disease and the trait was 2380 and 2480 grams. This 100 grams difference, however, was statistically insignificant.
Conclusion: Patients with sickle cell disease had more antenatal complications than those with sickle cell trait, without affecting the foetal outcome. Though the trait is generally considered a benign disease, women need special care and attention during a stressful situation like pregnancy.
Keywords: Sickle cell disease, Trait, Pregnancy, Complications, Outcome. (JPMA 63: 743; 2013).
Introduction
Sickle cell disease (SCD) is the most common haemoglobinopathy to complicate pregnancy. Sickle cell disorders afflict about 100 million people in the world with the highest prevalence in Nigeria. Pregnancy in women with SCD has been associated with increased frequency of medical and pregnancy-related complications.1
The effect of the carrier state, sickle cell trait (SCT), on pregnancy is less clear with conflicting evidence in the literature.2 Because of medical advances in obstetrics and neonatology, more women with SCD are attempting pregnancy.1 The life span for sickle cell patients in 1973 was 14 years. Three decades later, it increased to 50 years.1 Although maternal and perinatal mortality has recently been reported to be reduced for women with SCD, but they are still prone to several complications during pregnancy, including anaemia, severe crisis pulmonary disease and infections.4 Patients with SCT are rarely anaemic, usually asymptomatic and in good health. However, the stress of pregnancy modifies the situation. The sickling crisis in SCT women may occur in cases of extreme anaemia, dehydration, acidosis, vigorous exertion and at high altitude. SCD which affects 1 in 600 African Americans, is the most common haemoglobinopathy in the United States.5 Sickle cell gene is prevalent in 26% of the Saudi population. Earlier reports from this country indicated that sickle cell anaemia in pregnancy runs a relatively benign clinical course than elsewhere.6 Better management of this disease by taking care of patients since their birth has resulted in a significant reduction in morbidity and mortality in developed countries.7 Most studies of SCD in pregnancy document risks to the foetus that include pre-term labour and intrauterine growth restriction.8 There is limited data about maternal outcomes. The morbidity in sickler pregnant women is higher with an increase in sickling crisis in both antenatal and postnatal periods. There is also an increased risk of complications for the foetuses. Physiological changes during pregnancy predispose women to SCD-related complications and may explain the increased frequency of painful crisis during pregnancy.1 The current study was, therefore, carried out to compare the course and outcome of pregnancy in SCD and SCT women.
Patients and Methods
The retrospective, comparative study comprised records related to women who delivered at the Abha General Hospital, Abha, Saudi Arabia, from January 2009 to December 2011. All women with SCD and SCT were identified using the departmental registers. The medical records of these patients were reviewed for age, gravidity, parity, antenatal complications, sickle cell crisis, frequency of blood transfusion, mode of delivery, puerperium, intrauterine foetal death, perinatal and maternal morbidity, newborn\\\'s birth weight, gender and death. Pregnancy complications and foetal outcome in patients with SCD were compared with SCT patients.
Management of all the cases relevant to the study had been done according to the department\\\'s protocol for pregnant women with sickle cell disorders. This included frequent antenatal visits (fortnightly clinic visits till third trimester; then weekly), rigorous check for and treatment of infections on every visit, prevention and prompt treatment of specific complications such as crisis and blood transfusion with Hb-AA blood, when clinically indicated and/or when haemoglobin concentration dropped to <6g/dl. It also included regular antenatal foetal monitoring and intensive intrapartum and postpartum care of the women and their babies. Awaiting spontaneous onset of labour at term was the usual practice. Induction of labour and caesarean section was performed only for obstetric indications. Continuous foetal monitoring was carried out along with liberal oxygenation and hydration of the Hb-SS mothers to prevent crisis during labour. Significance of differences between the two groups of patients was assessed by chi-square test, Fisher\\\'s Exact test and student\\\'s t-test as appropriate. P-value <0.05 was considered statistically significant. The study was approved by the relevant institutional ethical and research committee.
Results
A total of 112 sickled pregnant women were identified during the study period. Out of them, 57 (50.89%) cases had SCD and 55 (49.10%) had SCT. Baseline characteristics of all the women in the two groups were noted and compared at the outset (Table-1).
There were 108 (96.42%) singleton and 4 (3.57%) twin pregnancies; 3 (75%) dichorionic-diamniotic twins, and 1 (25%) monochorionic-diamniotic twin pregnancy. Eight women were not delivered in our hospital, and were excluded from foetal outcome analysis. In the SCD group, there were 6 (10.52%) primigravida, and 6 (10.52%) women had more than one miscarriage. The corresponding figures for the SCT women were 11 (20%) and 12 (21.31%) respectively. The average haemoglobin (Hb) level in the SCD group was 8.35±1.12g/dl and in SCT women was 9.96±1.2g/dl. The commonest cause of hospital admissions in 45(79%) of the SCD cases was sickle cell crisis. Painful crisis was in 41(71.9%) and haemolytic crisis in 4 (7.01%) cases. The commonest complication, anaemia (Hb <10.5g/dl) was significantly high (p<0.001) in SCD cases: 55 (96.5%) versus 35(63.6%) in SCT women. Acute chest syndrome was found in 3(5.26%) SCD cases, while pregnancy-induced hypertension (PIH) was observed only in 4(7.27%) SCT women. Other complications of pregnancy were about equally common in both groups (Table-2).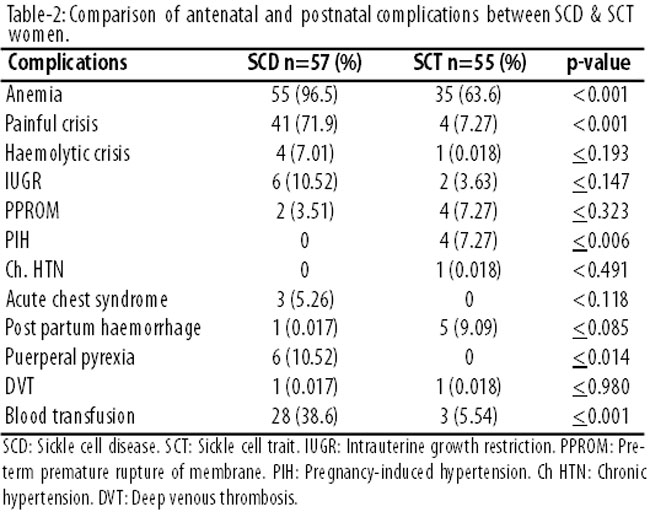
The gestational age was almost same in both groups. Regarding pregnancy outcome in SCD, 14 (28.57%) women ended in pre-term delivery (<37 weeks gestation) following spontaneous onset of labour versus 13(23.65%) patients of SCT group (Table-3).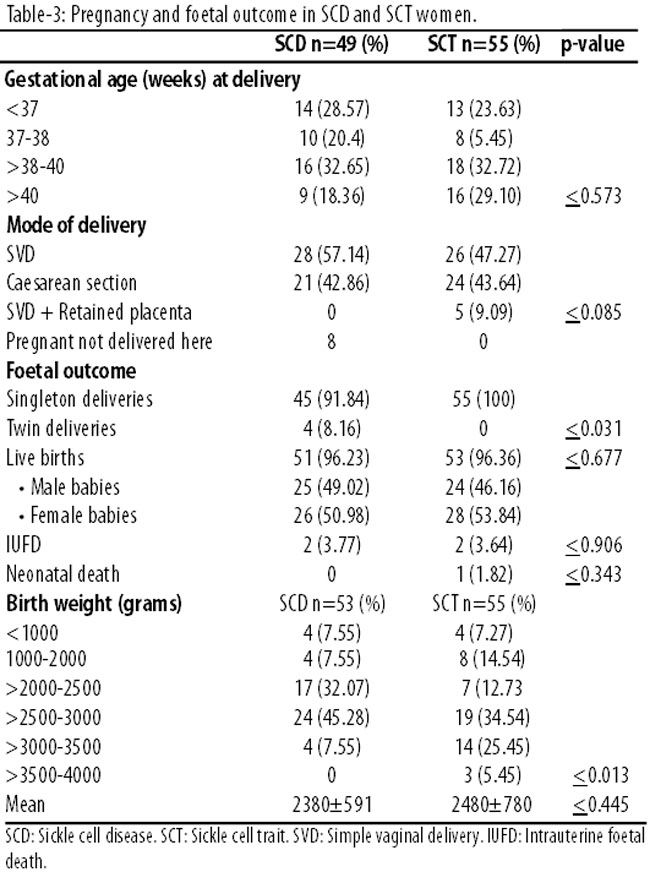
No obvious predisposing factor for pre-term delivery was found in any of these patients except 1 (0.96%) who had intrauterine foetal death (IUFD) prior to onset of labour. Average birthweight of babies delivered by SCD women was 2380±591 grams, and that of SCT women was 2480±780 gm. The 100 gram difference was statistically insignificant, but babies having birth weight >3000 grams were about 4 times more common in the SCT group. Delivery outcome was also almost similar in both groups.
Discussion
It is now well established that pregnancy with SCD has an increased risk of maternal and foetal complications.4,9 This study raises new concerns about SCD and Trait in pregnancy. SCT has been demonstrated to be associated with no additional risks to a woman in pregnancy, labour or puerperium, and not associated with any adverse outcome for neonates like stillbirth rate, intrauterine growth restriction (IUGR) and low birthweight (LBW). There is no significant difference between SCT group and general population.10 We dealt with more SCD women because they were expected to have more complications and were thus referred to our tertiary care hospital while probably most of SCT women were delivered in peripheral centres. Gravidity and parity in SCT women was higher (almost double) than SCD, probably because of parent\\\'s awareness of problems/complications and thus to avoid chances of having more SCD children. We found in our study that SCT women also have antenatal complications like anaemia, painful crisis, IUGR, PIH and LBW babies which are less frequent than SCD, but more than the general population. The reason why SCT have less twining compared to the SCD women in this study is unexplainable. It may require a look into the fertility pattern in an extensive research to throw light on to the issue. Regarding gestational age at delivery, mean gestational age in this study was 37.41±2.72 weeks which was the same as in another Saudi Arabian study, but different from a Nigerian study in which the mean gestational age was <37 weeks with higher incidence of pre-term deliveries.11,12 The frequency of complications during pregnancy like anaemia, painful crisis, haemolytic crisis, IUGR, puerperal pyrexia were observed higher in SCD than SCT women. These results conform to the findings of previous reports from this country.13 The disease appears to have less severe effect on Saudi mothers and babies compared to the outcomes reported from Nigeria and USA.14-16 The moderate effects of SCD in pregnancy in our patients was probably due to the hereditary persistence of a high percentage of Hb-F, which is protective against sickling.11,17 Anaemia was observed as one of the major complications of sickler patients, which is more marked in SCD (97%) compared to SCT (64%); similar to an earlier observation.11 In this study, 39% patients of SCD received blood transfusion, which was the same as in a Nigerian study.12 The intensity and frequency of sickle cell crisis is more pronounced during pregnancy. In this study, antenatal sickling complications were 72% in SCD compared to only 7% in SCT. This finding is not consistent with that of (45%) reported by a similar study in Saudi Arabia.11 This may be because of high altitude of our study region. Although women with SCD have been reported to have a higher risk of pre-eclampsia, but we did not observe this finding.4 Other studies have also corroborated our findings on pre-eclampsia, although like ours, their power was not sufficient to make firm conclusions.8,18 It would be interesting to examine this further in more robust prospective studies. In comparison with the general population, we did not find an increased risk IUFD in both groups, which was similar to that reported earlier.16 This may be attributed to improved foetal monitoring and the increased likelihood of proper, in-time interventions. Retained placenta has been reported as being more common in SCD by some studies, but this was not observed by us.18 In the current study, the frequency of retained placenta was found in 9% (5 cases) of SCT, but not at all in SCD. Sickle cell disease/trait both groups were associated with LBW babies. Average birthweight of all babies of the studied women was about the same as mentioned in a UK study and a Nigerian study.12,19 The neonatal birthweight difference between SCD and SCT groups of women was only 100 grams which was not statistically significant. The mean birthweight of babies of SCD (2380 grams) is lower than another Saudi study\\\'s finding (2750 grams).11 This may be due to chronic hypoxia at high altitude where pregnancies are associated with reduced oxygen delivery and density of placenta nutrient transporters. Furthermore, histopathology examination of placenta in SCD/SCT pregnancies revealed sickling in the intervillous space and decidual vessels suggesting hypoxia at maternal and foetal blood interface.21
Conclusions
The current study suggests that there is no significant difference in the course and outcome of pregnancy in SCD and SCT women. Although there have been remarkable improvement in the survival of such women during pregnancy, but they are still at a significantly increased risk of morbidity. A multidisciplinary team approach to deal with antenatal complications in SCD women will improve pregnancy outcome in these patients.
References
1. Hassell K. Pregnancy and sickle cell disease. Hematology/Oncology Clinics of North America 2005; 19:903-916. doi:10.1016/j.hoc.2005.07.003
2. Abdulsalam AA, Bashour HN, Monem FS, Hamadeh FM. Pregnancy outcomes among Palestinian refugee women with sickle cell trait in Damascus, Syria. Saudi Med J 2003; 24:986-90.
3. Claster S, Vichinsky EP. Managing sickle cell disease. BMJ 2003; 327:1151-5.
4. Smith JA, Espeland M, Bellevue R, Bonds D, Brown AK, Koshy M. Pregnancy in sickle cell disease: experience of the Cooperative Study of Sickle Cell Disease. Obstet Gynecol 1996; 87: 199-204.
5. Samuels P. Hematologic complications of pregnancy. In: Gabbe SG, Niebyl JA, Simpson JL, eds. Obstetrics: normal and problem pregnancies, 4th ed. Philadelphia: Churchill Livingstone, 2002; pp 1169-93.
6. El-Hazmi MA, Warsy AS, al-Swailem AR, al-Swailem AM, Bahakim HM. Sickle cell gene in the population of Saudi Arabia. Hemoglobin 1996; 20:18-98.
7. Lee A, Thomas P, Cupidore L, Serjeant B, Serjeant G. Improved survival in homozygous sickle cell disease: lessons from a cohort study. BMJ 1995; 311:1600-1602.
8. Sun PM, Wilburn W, Raynor BD, Jamieson D. Sickle cell disease in pregnancy: twenty years of experience at Grady Memorial Hospital, Atlanta, Georgia. Am J Obstet Gynecol 2001; 184: 1127- 30.
9. Thame M, Lewis J, Trotman H, Hambleton I, Serjeant G. The mechanisms of low birth weight in infants of mothers with homozygous sickle cell disease. Pediatrics 2007; 120:e686-93.
10. Adeyemi AB, Adediran IA, Kuti O, Owolabi AT, Durosimi MA. Outcome of pregnancy in a population of Nigerian women with sickle cell trait. J Obstet Gynaecol 2006; 26:133-7.
11. Al Jama FE, Gasem T, Burshaid S, Rahman J, Al Suleiman SA, Rahman MS. Pregnancy outcome in patients with homozygous sickle cell disease in a university hospital, Eastern Saudi Arabia. Arch Gynecol Obstet 2009; 280:793-797.
12. Afolabi BB, Iwuala NC, Iwuala IC, Ogedengbe OK. Morbidity and mortality in sickle cell pregnancy in Lagos, Nigeria: A case control study. J Obstet Gynaecol 2009; 29:104-6.
13. Perrine RP, John P. Pregnancy in sickle cell anemia in a Caucasian group. Am J Obstet Gynecol 1974; 118:29-31.
14. Ogedenghe OK, Akinyanju O. The pattern of sickle cell disease in pregnancy in Lagos, Nigeria. West Afr J Med 1993; 12:96-100.
15. Omo-Aghoja IO, Okonofua FE. Pregnancy outcome in women with sickle cell - a five year review. Niger Postgrad Med J 2007; 14:151-4.
16. Villers MS, Jamison MG, Castro LM, James AH. Morbidity associated with sickle cell disease in pregnancy. Am J Obstet Gynecol. 2008; 199:125.e1-5.
17. Al Awamy BH, Niazi GA, El-Mouzan MI, Al Torki MT, Naeem MA. Newborn screening for sickle cell hemoglobinopathy and other inherited erythrocytic disorders in the Eastern Province of Saudi Arabia. Saudi Med J 1986; 7:502-509.
18. Serjeant GR, Loy LL, Crowther M, Hambleton IR, Thame M. Outcome of pregnancy in homozygous sickle cell disease. Obstet Gynecol 2004; 103:1278-85.
19. Tan TL, Khanapure A, Oteng-Ntim E. Sickle-cell trait and small-for-gestational age babies: Is there a link? J Obstet Gynaecol 2008; 28:298-300.
20. Zamudio S, Baumann MU, Illsley NP. Effects of chronic hypoxia in vivo on the expression of human placental glucose transporters. Placenta 2006; 27:49-55.
21. Taylor MY, Wyatt-Ashmead J, Gray J, Bofill JA, Martin R, Morrison JC. 2006. Pregnancy loss after first-trimester viability in women with sickle cell trait: time for a reappraisal? Am J Obstet Gynecol 2006; 194:1604-8.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: