
Abid Hussain Laghari ( Section of Cardiology, Department of Medicine, Aga Khan University Hospital, Karachi. )
Javed Majid Tai ( Section of Cardiology, Department of Medicine, Aga Khan University Hospital, Karachi. )
May 2013, Volume 63, Issue 5
Case Reports
Abstract
A middle-aged male presented with symptoms of exertional shortness of breath and leg swelling for the past six months. Examination revealed raised jugular venous pressure (JVP), pitting pedal oedema, muffled heart sounds, bilateral pleural effusion and hepatomegaly. Echocardiogram showed features of constrictive pericarditis with heavily thickened pericardium, which was confirmed by cardiac computed tomography (CT). The patient underwent pericardiectomy following which echocardiographic features of constriction were reversed and the patient became asymptomatic.
Keywords: Pericarditis, Constrictive, Echocardiography, Pericardiectomy.
Introduction
Constrictive pericarditis is a rare condition characterised by clinical signs of right heart failure subsequent to loss of pericardial compliance. The aetiology of constrictive pericarditis has changed during the last decades in the developed countries. Tuberculosis (TB) accounted for 49% of the cases of constrictive pericarditis in a series reported in 19621 but cardiac surgery has become one of the main reasons for its development in recent years. TB is still the frequent cause of constrictive pericarditis in developing countries because the relative incidence of TB as a cause of pericardial disease is associated with the overall prevalence of TB in a given population. TB pericarditis occurs in 1 to 2% of patients with pulmonary TB.2 However, cases defined as idiopathic constrictive pericarditis are still seen.
Case Report
A 64-year-old male, with known history of diabetes mellitus and hypertension, presented in the cardiology clinic with complaints of progressively increasing shortness of breath on exertion for the past 6 months, but no history of chest pain, fever or cough. On examination, he had a pulse of 96 beats/minute regular, blood pressure of 115/75 mmHg, raised jugular venous pressure (JVP), and pitting pedal oedema. His heart sounds were muffled. There was dull percussion note and bilateral decreased breath sounds at lung bases along with enlarged liver but no ascites. Bilateral pleural effusion was found on chest x-ray and low voltage was found on electrocardiography (ECG).

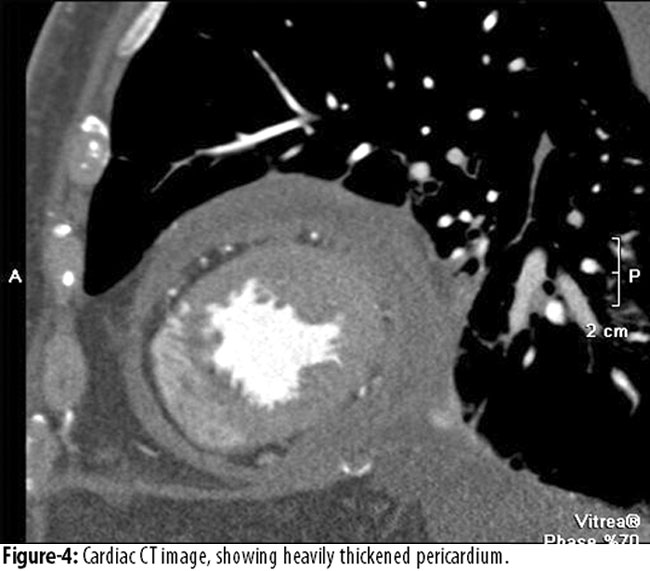
The echocardiogram showed abnormally thickened pericardium (18 mm) with trace circumferential pericardial effusion, biatrial enlargement and normal left ventricular systolic function. Septal bounce was noted, along with non-collapsing dilated inferior vena cava and expiratory diastolic reversal in hepatic vein. A cardiac CT angiogram was performed which reconfirmed the finding of a heavily thickened pericardium and normal coronaries.
Autoimmune workup was negative. The patient underwent pericardiectomy, and pericardial tissue acid-fast bacilli (AFB) smear and culture were found to be negative. Histopathology of pericardial tissue was inconclusive and did not show any caseous granulomas. After pericardiectomy, the echocardiographic features of pericardial constriction were reversed and the patient became asymptomatic.
Discussion
The clinical presentation of constrictive pericarditis may vary, as noted in a series of 135 patients, in which 67% of the patients presented with heart failure, 8% with chest pain, 6% with abdominal symptoms, 4% with atrial arrhythmia, and only 5% with cardiac tamponade.3 The risk of developing constrictive pericarditis following the first episode of acute pericarditis was evaluated prospectively in 500 patients over a mean follow-up time of 6 years (24 to 120 months).4 Constrictive pericarditis developed in 1.8% of the total patients.4 Case reports of constrictive pericarditis following orthotopic heart transplants have also been published.5 Tuberculosis accounted for 49% of the patients of constrictive pericarditis in a case series reported in 1962.1 TB is still a common cause of constrictive pericarditis in endemic areas and in patients with human immunodeficiency virus (HIV) infection, but only a rare cause in developed countries. Effusive constrictive pericarditis, though itself relatively uncommon, is mostly caused by tuberculosis. Chest x-ray showing calcification around the heart is strongly favourable for constrictive pericarditis in patients with signs and symptoms of right-sided heart failure.6 Transthoracic echocardiography is a very important diagnostic test for constrictive pericarditis evaluation — 2D and M-mode for structural visualization and Doppler echocardiography for haemodynamic assessment.6 In a reported series of 143 surgically confirmed cases, increased pericardial thickness was seen in 37% of the cases, abnormal septal motion in 49%, and atrial enlargement in 61%.7 Cardiac CT is superior to cardiac magnetic resonance (CMR) in detecting calcification, but CMR better differentiates small effusions from pericardial thickening. CMR can assess haemodynamic events like septal bounce, as well as identify pericardial inflammation and pericardial-myocardial adherence.8 The late gadolinium enhancement (LGE) of the pericardium seen on CMR is fairly common but not universal in constrictive pericarditis and might be a predictor of reversibility following treatment.9 Invasive haemodynamic assessment is rarely needed to confirm the diagnosis of constrictive pericarditis, otherwise it is mainly used in situations of suboptimal or non-diagnostic echocardiographic findings, or for evaluation of coronary anatomy prior to pericardiectomy. The signs and symptoms of constrictive pericarditis are usually progressive in majority of the patients unless treated surgically with pericardiectomy. Sometimes, the signs and symptoms of constriction are transient or reversible in a minority of patients with constrictive pericarditis. Therefore, in the absence of features like cachexia, atrial fibrillation, hepatic dysfunction, or pericardial calcification which indicate that the constrictive pericarditis is chronic, newly diagnosed patients who are haemodynamically stable may be given a trial of conservative management for 2 to 3 months before pericardiectomy. Pericardiectomy is the only definitive treatment, and medical therapy such as diuretics may be used as a temporising measure, or for patients who are not candidates for surgery. Patient outcomes are best at high volume centres with greater experience of pericardiectomy. In patients who underwent pericardiectomy between 1970 and 1985, the operative mortality was 12%, but significantly lower mortality rate between 4 to 8% was reported in patients who underwent pericardiectomy between 1977 and 2006.10
Conclusion
Constrictive pericarditis is a rare condition characterised by clinical features of right heart failure. TB is the frequent cause of constrictive pericarditis in developing countries whereas cardiac surgery is the most common cause in developed countries. Cases defined as idiopathic constrictive pericarditis are still seen as was the case in our patient.
References
1. Robertson R, Arnold CR. Constrictive pericarditis with particular reference to etiology. Circulation 1962; 26: 525-9.
2. Larrieu AJ, Tyers GF, Williams EH, Derrick JR.Recent experience with tuberculous pericarditis. Ann Thorac Surg 1980; 29: 464-8.
3. Ling LH, Oh JK, Schaff HV, Danielson GK, Mahoney DW, Seward JB, et al. Constrictive pericarditis in the modern era: evolving clinical spectrum and impact on outcome after pericardiectomy. Circulation 1999; 100: 1380-6.
4. Imazio M, Brucato A, Maestroni S, Cumetti D, Belli R, Trinchoro R, et al. Risk of constrictive pericarditis after acute pericarditis. Circulation 2011; 124: 1270-5.
5. Bansal R, Perez L, Razzouk A, Wang N, Bailey L. Pericardial constriction after cardiac transplantation. J Heart Lung Transplant 2010; 29: 371-7.
6. Maisch B, Seferovic PM, Ristic AD, Erbel R, Rienmüller R, Adler Y, et al. Guidelines on the diagnosis and management of pericardial diseases executive summary; The Task force on the diagnosis and management of pericardial diseases of the European society of cardiology. Eur Heart J 2004; 25: 587-610.
7. Talreja DR, Edwards WD, Danielson GK, Schaff HV, Tajik AJ, Tazelaar HD, et al. Constrictive pericarditis in 26 patients with histologically normal pericardial thickness. Circulation 2003; 108: 1852-7.
8. Verhaert D, Gabriel RS, Johnston D, Lytle BW, Desai MY, Klein AL. The role of multimodality imaging in the management of pericardial disease. CircCardiovasc Imaging 2010; 3: 333-43.
9. Feng D, Glockner J, Kim K, Martinez M, Syed IS, Araoz P, et al. Cardiac magnetic resonance imaging pericardial late gadolinium enhancement and elevated inflammatory markers can predict the reversibility of constrictive pericarditis after anti-inflammatory medical therapy: a pilot study. Circulation 2011; 124: 1830-7.
10. Chowdhury UK, Subramaniam GK, Kumar AS, Airan B, Singh R, Talwar S, et al. Pericardiectomy for constrictive pericarditis: a clinical, echocardiographic, and hemodynamic evaluation of two surgical techniques. Ann Thorac Surg 2006; 81: 522-9.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: