
Nargese J. Talati ( Department of Obstetrics and Gynaecology, Lady Dufferin Hospital, Karachi. )
October 1998, Volume 48, Issue 10
Original Article
Abstract
A hospital based epidemiological study of benign gestational trophoblastic disease i.e., both complete and partial hydatidiform mole was undertaken at 8 hospitals. The frequency of the disease was found to be 3.8911000 pregnancies and was found to be higher - 1 in 237 deliveries in the economically deprived women admitted to a free Government Hospital, compared to only I in 471 deliveries in a Private, fee-for-service hospital. Risk factors identified, were: age above 35 years (OR=7.39, CL 5.54 -9.87); or under 20 years (OR=2.14, CL=1.60-2.85), history of previous molar pregnancy (OR=18.44, CL=49.4-74.09), past history of abortions (OR=1.96, CL=l.49-2.57) and recurrent abortions (OR=3.26, CL=1.82-5.77). Blood group A was also found to be a significant risk factor (OR=1.6, CL=I.01-2.53). Progression to gestational trophoblastic tumor was found in 3% patients with hydatidiform mole. A plea is made for earlier diagnosis at asymptomatic stage, to reduce morbidity; histopathological examination of all abortuses will help identify complete and partial moles which would otherwise be overlooked. Finally, improvement in follow-up system and establishment of a data base is recommended (JPMA 48:296,1998).
Introudction
Gestational trophoblastic disease (GTD) is relatively rare in the West but found with higher frequency in South East Asia1,2. Benign GTD i.e., hydatidiform moles (HM) are either complete or partial. They are genetically and morphologically different entities. The complete moles (CM) are characterised by the absence of an embryo, genemlised hyperplasia of both syncitio and cyto- trophoblast and villous edema. Genetically they are usually 46XX - the result of fertilization of an anucleate egg with a sperm that reduplicates itself. If there is disperrny as occurs in a small sub-set, the genotype would be 46xY3,3a. The partial mole (PM) have some hydropic villi in addition to nonnal ones which can support fetal existence for some time. It is usually Triploid3. The importance of HM is obvious as in over 60% of malignant GTD, the antecedant pregnancy is a HM. Secondly, it can cause considerable morbidity.
Patients and Methods
In order to determine the frequency of HM in Karachi, an epidemiological study was undertaken, to assess quantitatively, the risk factors and clinical features of the disease and compare them with those of trophoblastic disease centres in other parts of the world. In this case control study, data was collected retrospectively from 8 hospitals in Karachi, i.e., Agha Khan University Hospital, Jinnah Post Graduate Medical Centre, Lady Dufferin Hospital, Liaquat National Hospital, Lyari General Hospital, P.N.S. Shifa, Seventh Day Adventist Hospital and Ziauddin University Hospital. These eight hospitals situated in three districts of Karachi South, Central and East and represent a cross section of a widely differing patient population from the economically deprived and illiterate patients to the elite educated class. A questionnaire was sent to all hospitals and data collected by retrospective analysis of case files. Clinical features,
laboratory investigations results and treatment instituted was recorded. The diagnosis of CM was made on macroscopic examination but that of PM was confirmed by histopathology. The controls were 8,226 gravidas delivering after28 weeks, at the LDH in a two year period.
Several sociodemographic variables were chosen to identify the risk factors and the calculated Odds ratio was used as an estimate of relative risk.
Results
Data was available for 413 patients with HM during which time there were 96,400 deliveries giving a frequency of 1 in 233 deliveries. The effect of change in denominator from ‘deliveries’ to ‘pregnancies’ - (i.e., abortions, ectopic pregnancies in addition to live and stillbirths) is readily seen in data from 4 hospitals where the frequency was 1 in 216 deliveries but only 1 in 257 pregnancies i.e., 3.89/1,000 pregnancies (Table I).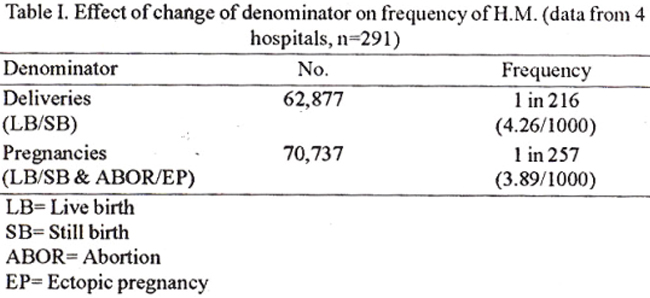
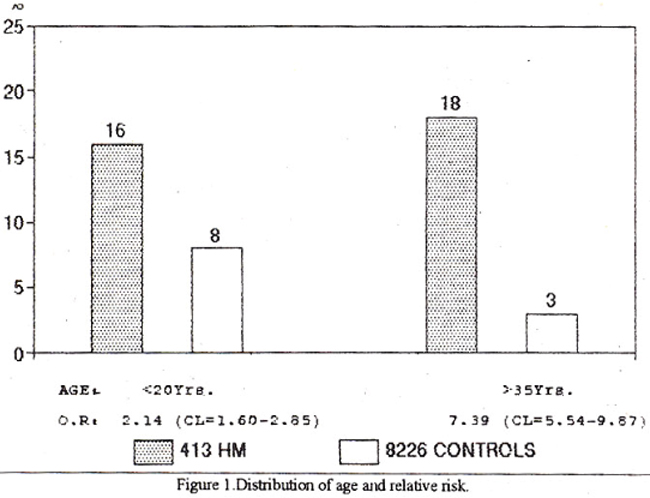
Figure 1 shows distribution of age and relative risk with odds ratio for women <20 years to be 2.14 and for women >35 years it was 7.39.
Reproductive factors.
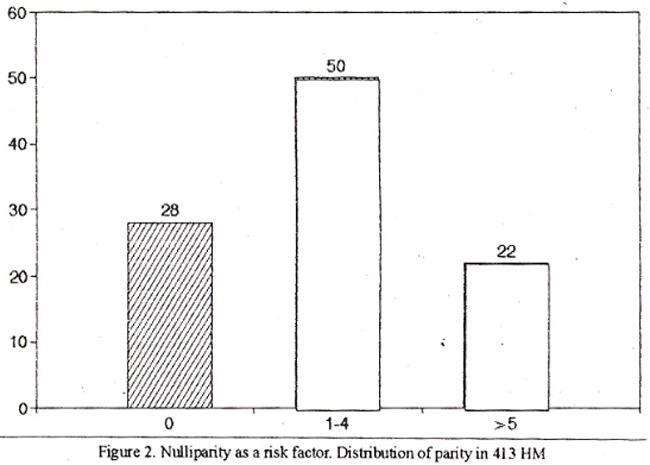
Figure 2 shows the distribution of parity, 28% being Nulliparous women. Women who have had an abortion in the past are at greater risk (OR 1.96) (Figure 3)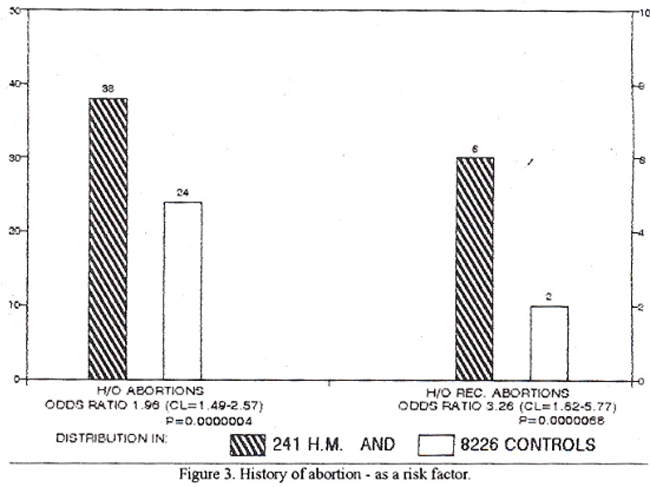
and with recurrent abortion the risk of H.M. rose to 3.26. Data was available for 116 patients with a history of previous H.M. Eight had a positive history, the recurrence rate being 7% and the odds ratio was 18.44.
There was a positive history of intrauterine insemination with husband’s semen, in only one among 413 cases.
The clinical features revealed that 53 percent patients presented with a uterus larger than expected from gestational age (GA), majority (68%) had a GA of 13-20 weeks, 5% were over 20 weeks and only 27% presented at <12 weeks. There were however wide variations in data from different hospitals, with regard to both these features. The results of ultrasound in the diagnosis of HM was available in six hospitals only where 135 patients were scanned. The diagnosis was correct in 87%. Asymptomatic HM i.e., a diagnosis (on the basis of ultrasound scan) before the occurrence ofbleeding was made in 4% of 204 cases. Hyperemesis was present in 22% and one each had preeclamptic toxaemia (PET) and acute pulmonaiy symptoms. Theca Lutein Cysts were reported in 29 out of 204 HM patients (i.e., 14%) in data available from 5 hospitals. Partial mole was reported in a higher frequency of 74% with the overall figure being 21%.
Details of B.HCG were available for 81 patients from two hospitals and showed that 71% had titres between 104 and 105 25% had low litres of <104 and in only 4% were the levels However, from AKUH (where specimens were analysed in their own lab.) the mean litre in 29 patients was 200,649 mIU/ml. Information on blood group was available from 4 hospitals only.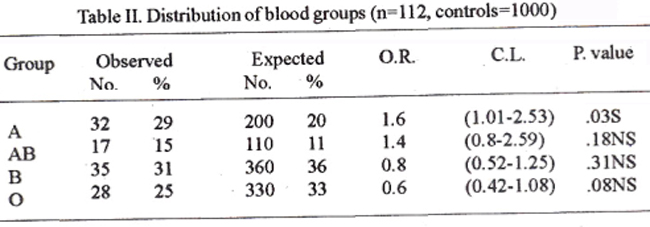
Table II shows a slight preponderance of groups A (OR=1.60) and AB (OR=1.45) over controls. However, the P value for group A was significant and that for AB was not. Suction evacuation was the treatment of choice carried out in 97% cases, 3% underwent hystrectomy which was performed prior to 1993.
Immediate morbidity was assessed by the quantity and duration of blood loss and the need for transfusion. Nine percent patients presented within 24 hours of onset of bleeding, 49% between 1-10 days and 42% between 10 days and 3 months. Forty-one percent patients had a Hb less than 10G% on admission and blood transfusion was necessary in 48%. Thirty-seven percent cases required 1-2 units and 11%, 3 or more units. Progiessionto gestationaltrophoblastic tumor with need for chemotherapy was reported in 13 out of 413 patients on follow-up (3%).
Discussion
This study shows frequency of benign gestational trophoblastic disease to be 3.89/1000 pregnancies for the city of Karachi - markedly less than in Indonesia (11.7/1000) and about four times that inUK and US (0.7/1000)1. The Middle East - Iraq’s frequency (4.5/1000) is almost similar to ours, but that of S. Arabia is 2.2/10002 (Figure 4).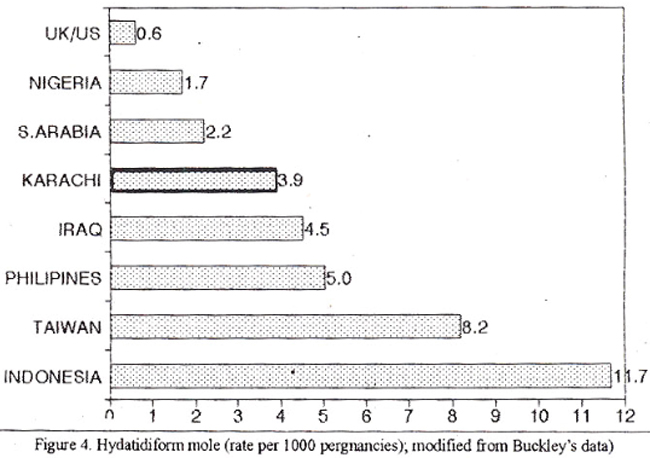
As this is a retrospective analysis of case records that were available, the possibility of under reporting is present. It was also realised that hospital based data could be biased, but this analysis would indicate the pattern of GTD in Karachi.
Of the various parameters studied, age was found to be a significant risk factor at both ends of reproductive life and the relative risk for the teenager was 2.14. Several trophoblastic disease centres in US3, Singapore4, Italy5, Israel6, UK7 and Hawaii8 have reported an increased risk in the below 20 age group. Similarly this study showed the relative risk for women >35 years tobe 7.39. Parazzim5 confinned an increased risk in women over 40 and Yen9found the risk tobe 25 times over the age of45 and at the age of49 years; Bagshawe10 found the risk to be 200 fold. A study from the Milan Trophoblastic Disease Centre5 found an increased risk associated with nulliparity, a history of spontaneous abortion and difficulty in conceiving.
Nulliparity (28% cases) was found to be a risk factor for GTD in this study; a similarfigure has been quoted from Saudi Arabia (3 1%)2. A histoiy of previous abortions was the second risk factor with 3.2% in recurrent abortions. Parazzini5 found the risk to be 3.1. It is possible that a high incidence of abortions in molar patients may suggest chromosomal disorders in the conceptus. Lawler’s cytogenetic studies10 showed that women with FIM had 4 times more balanced translocations. This increases the chance of upsetting the meiotic process resulting in an anucleate egg, leading to either an abortion or HM in a continuum of reproductive failure. We found a high recurrence rate of 7% when there had been a previous molar pregnancy. Others have reported recurrence rate of 1.511 and 2%12. Several other authors5,6,9,13 have calculated a RR of between 18 and 40, similar to our findings.
In Australia Olesnicky5 found an increased risk after Intrauterine Insemination (Donor Semen) - there was a single case following AIH in this series. In the clinical features studied, it was significant that in 73% the diagnosis was not established till the second trimester and that in 53% the uterus was “large- for dates”. Berkowitz14 and Curry15 found a positive association between the large size of uterus in addition to G.A. of >10 weeks and the risk of malignant sequelae and of course the immediate morbidity would increase because evacuation is more likely to be associated with greaterblood loss and greater need forblood transfusion.
The role of socioeconomic factors in the frequency and morbidity of H.M. is controversial. Although most authors agree that there is an increased frequency in the economically deprived women e.g., in S.E. Asia1,2,8-10. On the other hand a relatively low frequency is seen in the affluent Kingdom of S. Arabia2.
It is common knowledge that Gynecologists in Karachi see very few cases of GTD in their private practice while it appears to be more common in the general ward patients. Although itwas not possible to obtain data on patients income, the social status was inferred from whether she was treated in a free hospital or a fee-for-service hospital. The frequency of H.M. in JPMC which treats poor patients free of charge was 1 in 237 deliveries, whereas in SDA hospital which caters mostly to the upper classes it was 1 in 471 deliveries. Further, at JPMC, 79% of patients had a “large for dates” uterus and 81% of LDH patients were diagnosed in second trimester. AKUH had only 15% patients with a “large-for-dates” uterus and the mean age at diagnosis was 11.5 weeks.
It would be hypothesized that since affluence also determines access to food, the calorie and protein intake are diminished in the poor. Compared to a daily protein intake of 87G in France, 76G in Netherlands and 88G in S.Arabia2, the mean protein intake in Pakistan (according to Govt. of Pakistan National Nutritional Survey’85-87) is only 610. But patients who could afford private tertiaiy hospital care had normal nutritional parameters15.. Reports from Taiwan, Mexico and Philippines have suggested low protein intake as an etiological factor10. However, other studies have refuted this hypothesis - as the lnnuits of Alaska, inspite of a diet of mainly game and fish, have a high incidence of H.M10.
Although anaemia was present in 41% patients, only 48% required blood transfusion. Data from different hospitals varied widely - e.g., PNS Shifa which treated 86% of low income patients - had 82% prevalence of anaemia and 72% were transfused.
Delay in diagnosis was frequent -42% presenting with bleeding of long duration and in 48% the bleeding was moderate or severe. The reason could have been the patient’s apathy towards hospitalization with initial treatment by Traditional Birth Attendants, or to late reffermi by the family doctors and sometimes to the confusing clincial picture, ultrasound and histopathology reports. The need for early diagnosis is obvious, if morbidity is to be reduced.
Ultrasound has been accepted as a sensitive and reliable method of diagnosis of H.M. and a correct diagnosis was obtained in875 cases. Szulmannand Surti3 have demonstrated a linear relationship between the size of vesicles and the G.A. Thirteen percent false negatives inthis study may partly be due to failure to identify the veiy small vesicles of a very early pregnancy. This study compares favourably with ‘95 Boston study16 where false negative were 29%. The same study showed a pick-up rate of 9% of asymptomatic cases, whereas it was only 4% in this study. Routine ultrasound examination in early pregnancy would be helpful in diagnosis of H.M. before the onset of bleeding. This has already been achieved in the case of ectopic pregnancy where early ultrasound diagnosis before tubal rupture has helped reduce morbidity.
The incidence of Theca Lutein Cysts of 14% in this study, is lower than the 20% reported by Curry11,12 and others. The cysts may occasionally increase morbidity, if they undergo torsion - requiring emergency surgery and if they persist after evacuation may point to a possibility of persistent trophoblastic disease.
Partial moles are distinct, genetically and morphologically from complete moles. Begshawe7 and Parazzini5 have reported figures of 28% and 26% respectively using both histopathological and cytogenetic criteria. The frequency in this study was 21% using only histopathological criteria. There appears to be a strong possibility of under reporting, as only 3 hospitals had facilities to examine all specimens. Thus many H.M. in the abortions may have escaped detection and many apparently CM may have been PM. Bagshawe17 has emphasized the importance of distinguishing a molar from a normal conceptus by histopathology - as the patients’ future depends on this distinction.
Although the overall frequency of abortions in this study was 21%, one hospital (AKUH) reported a figure of 74%. It is interesting that a morphologic and cytogenetic study in Hawaii8 of spontaneous abortions found a prevalence of 68% P.M. Bagshawe17 found under reporting (14%) in UK before 1988, which changed later to over reporting (28%). Later still, on re-examination, many of these were reclassified as CM with the help of flow cytornetry. The diagnostic dilemma will remain until criteria are improved18 and flow cytometry available19,20.
The Triploid PM has a reduced propensity to malignant sequelae the risk being 1 in 200 compared to 1 in 12 for CM. A study of gestational trophoblastic tumor from Taiwan21 found the antecedant molar pregnancy to be CM in 62% and PM in only 2.9%. Bagshawe17 7. Rice and Szulmann have reported gestational trophoblastic tumor after a PM to be essentially non-metastatic, although metastasis has been reported from Taiwan in 2 out of 6 cases22. Although the real risk of malignamcy with PM is small, all cases need to have a follow-up17 and in the rare sub-set of diploid PM, where the fetus can survive23, the prognosis for the patient is worse because of its greater malignant potential.
Th BHCG titres varied widely according to whether the specimen was examined in the hospital’s own lab, or was sent to an outside lab. In the latter case the titres were lower probably due to deterioration of the BHCG during transport -emphasizing the need to use insulated containers for transporting specimens.
Although Chattopadhyay2 found a preponderance of blood group 0 in the Riyadh study, the Milan study found a preponderance of group A and AB. Several others studies1,22,24 have reported an excess of group A in molar patients, similar to our findings. In this study there were no hysterotomies or medical inductions; 97% patients had a suction curettage as the primary treatment. Although there may be the occasional place for a hystrectomy23,24, e.g., in a grand multipara over 40 years, the practice of prophylactic hysterectomy is now abandoned as it does not prevent malignant sequelae12. It is of interest to note that all nine hystrectoniies in this series were performed prior to 1993. The incidence of progression to gestational trophoblastic tumor and need of chemotherapy has been reported as 5.6% in UK and 26% in US7 but was only 3% in this study, probably because many of the patients were lost to follow-up.
The need for earlier diagnosis to reduce this morbidity is emphasized. Routine performance of histopathology on all abortuses may reveal higher figures of GTD than that reported here. A prospective study would provide improved data and a more close follow-up of the cases is necessary which could be achieved by instituting a data base.
References
1. Buckley JD. The epidemiology ofmolar pregnancy and choriocarcinoma” Clin. Obstet. Gynecol., 1984;27: 153.9.
2. Chattopadhyay S. Sengupta BS, Al-Ghreimil Met al. Epidemiological study of gestational trophoblastic disease in Saudi Arabia. Surg. Gynecol. Obstet., 1988;167:393-7.
3. Szulman AE, Surti U. Syndromes of HM. Cytogenetic and morphologic correlations. Am. J. Obstet. Gynecol., 1978; 131:665-71.
3. Szulman AE and Surti U. Syndromes of hydatidiform mole: Morphologic evolution of complete and partial mole. Am. 3. Obstet. Gynecol., 1978; 132:20-27.
4. Tech ES, Dawood MY. Ratnam SS eta!. Epidemiology ofhydatidiform mole in Singapore. Am. 3. Obstet. Gynecol.. 1971; 110:415-20.
5. Parazzini F. Mangili C, Vecchia CL. Risk factors for gestational trophoblastic disease: A separate analysis of complete and partial moles. Obstet. Gynecol. 199 1;78:1039-45.
6. Matalion M, Modan B. Epidemiological aspects of hydatidiform mole in Israel. Am. J.. Obstet. Gynecol., 1972;112:107-12.
7. Stone M, Bagshawe KD. An analysis of influence of maternal age, gestational age, contraceptive method and the mode of primary treatment of patients with hydatiform moles, on the incidence of subsequent chemotherapy. Br.J. Obstet. Gynecol., 1979;86:782-92.
8. JacobsPA, Hunt PA, Matsuura JS eta!. Complete andpartial hydatidiform mole in Hawaii: cytogenetics, morphology and epidemiology. Br.J. Obstet. Gynecol, 1982;89:258-66.
9. Yen 5, MacMohon B. Epidemiological features of trophoblastic disease. Am. J. Obstet. Gynec., 1968;101:126-32.
10. WHO Bulletin No.692. 1983. Gestations! trophoblastic disease. Technical reportseries. Geneva, WHO, 1983.
11. Vassilakos P, Rioton G, Kajii T. Hyditidiform mole: Two entities. A morphologic and cytogenetic study with some clinical considerations. Am. J. Obstet. Gynecol., 1977;127:167-70.
12. BrackenMB. Incidence and etiology ofhydatidiformmole: An epidemiotogical review. Br. J. Obstet. Gynecol., 1987;94:1123-35.
13. Howard Jones III, ln Novek\\\'s text book ofGynecotogy, edited by HW Jones AC, Wentz LS.Brunett.
14. Berkowitz RS, Crammer DW, Bemstein MR et al. Risk factors for completc molar pregnancy from a case control study. Am. J. Obstet. Gynecol. 1985;152:1016-20.
15. Curry S, Hammond CB, Tyray L et sI. Hydatidiform mole - Diagnosis, management and longtime follow-up of 347 pstietns. Obstet. Gynecol., 1975;45:1-8.
16. Wright VS. Bernstein M, Goldstein D et al. Changing presentation of complete molar pregnancy. Obstet Gynecol., 1995;86:775-9.
17. Bagshawe KD, Lawler SD, Paradinas FJ et al. Gestational trophoblastic tumors following initial diagnosis of partial mole. Lancet, 1990;335: 1074-76.
18. Hemming D, Quirke P, Womak C et al. Diagnosis of molar pregnancy and persistent trophoblastic disease by flow cytomctery. I. Clin. Pathol., 1987;40:615-20.
19. Lawler 5, Fisher R, Dent J. A prospective genetic study of complete and partiat hydatidiform moles. Am. I. Obstet. Gynecol., 1991;164:1270-77.
20. Howat Al, Beck 5, FoxH et al. Can histopathologiats reliably diagnose molar pregnancy? I. Clin. Pathol., 1993;46:599-602.
21. Chen RI, Huang SC, Chaw SN et al. Persiatant geatational trophoblastic tumor with partial mole as antecidant pregnancy. Br. I. Oh. & Gyn., 1994;101:330-34.
22. Crooij MlJ, VanderHarten JJ, Puyenbroek JI et al. A partial hyditidiformmole dispersed throughout the placenta, co-existing with a normal living fetus. Br. J. Oh. Gyn. 1985;92:104-6.
23. Sen DK, Ratnam 55. Gestational trophoblastic disease in contributions to obstetrics and gynecology Vol.1, 1991 Ed. SS. Ratnam and Soon Chye Ng.
24. Dawood MY, Tech ES, Ratnam SS. ABO Blood group in trophoblastic disease. I. Obstet. Gyne, BrCommon. 1971;78:918-23.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: