
Muzammil Hasan Najmi ( Department of Pharmacology and Therapeutics, Army Medical College, Rawalpindi. )
Rehan A. Hafiz ( National Institute of Health, Islamabad. )
Inayat Khan ( WHO, Geneva, Ministry of Islamabad. )
F.R.Y. Fazli ( Health, Geneva, Ministry of Islamabad. )
March 1998, Volume 48, Issue 3
Original Article
Abstract
The extent and nature of irrational prescribing of drugs has not been explored in Pakistan A pilot study was therefore undertaken in three major teaching hospitals located in the twin cities of Rawalpindi/Islamabad. Six hundred and one prescriptions from medical, paediatrics and psychiatry units of these hospitals were analyzed to study the prescribing pattern. The mean number of drugs per prescription was found to be 2,97. Only 23.6% drugs were prescribed by their generic names, About 80% of the prescribed drugs were from the National Essential Drug List of Pakistan. Use of injectable preparations was 17.1%, Antimicrobials constituted 20.4% of the drugs prescribed, frequently for cases of acute respiratory infections and gastroenteritis. The average cost of treatment per day was Rupees 26.10 in the outdoois and Rs 88.36 in indoois. Treatment did not correlate to the diagnosis in 24.6% of the cases. Doses of drugs were inappropriate in 30.6% prescriptions. Duration of treatment was not specified on a vast majority (73.4%), of the prescriptions. The data highlights the need for educational, managerial and regulatory interventions to rationalize the drug use in Pakistan (JPMA 48:73,1998).
Introduction
Irrational prescribing is a global problem, particularly affecting the developing countries1. The enormous developments taking place in the fields of pharmacology, phannaceutical chemistiy and pharmacy have resulted in a drug-explosion over the past few decades. An exponential increase in the number of available drugs has altered the ways in which the drugs are developed, presented and protected by law. The expansion of therapeutic arsenal also reflects the pressures exerted by drug manufacturers, seeking to ensure a constant expansion of their market2. The use of drugs is a specialized art requiring knowledge and experience. In addition there are non-medical factors that may influence the prescribing pattern3. Drugs are usually not used to their full potential or according to the generally accepted criteria. The physicians are subjected to positive and negative pressures from peers and patients and are also exposed to commercial persuasion.
There may be a striking variation in the pattern of drug use from country to country and in different areas of an individual country4. Even in developed countries like USA possessing an elaborate medical facility, the prescribed treatment was not found to correlate with the diagnosis in 20-40% cases5,6. Generalized irrational drug utilization involving marketing, distribution, prescribing, dispensing and use of drugs further aggravates the situation in less developed countries7.
Drug utilization has been defined by WHO8 as the marketing, distribution, prescription and use of drugs in a society with special emphasis on resultant medical, social and economic consequences. in the prevailing drug scenario, drug utilization studies have emerged as an important tool to find out the overuse, underuse or misuse of individual drugs or therapeutic classes of drugs in a society9. The experience from developed countries has provided evidence that drug utilization based operational research is valuable for the provision and maintenance of adequate pharmaceutical services matching the needs of the majority of population10.
The present study was, therefore, planned to assess the prescribing pattern in three major teaching hospitals in the twin-cities of Rawalpindi/Islamabad, which contribute greatly to the prescribing practices for a large segment of the medical profession.
Materials and Methods
The study was conducted in the Internal Medicine, Paediatncs and Psychiatry units of Pakistan Institute of Medical Sciences Islamabad, Rawalpindi General Hospital and Military Hospital Rawalpindi.
Sampling: Sampling of prescriptions was carried out from September to November, 1995. Prescriptions were randomly collected from out-patient and in-patient departments of the participating units. The sample size from any individual unit ranged from 30 to 84 depending upon availability. The sampling was carried out prospectively in case of outdoor departments, while it also included the retrospective record of the indoor patients. The whole procedure was completed with consent of authorities of the concerned institutions and confidentiality of the prescriptions was strictly maintained.
Parameters Studied: Each individual prescription was analyzed on a proforma designed in the light of drug-use indicators suggested by the WHO11, for the following parameters.
a. Total number of drugs in the prescription.
b. No. of drugs prescribed by generic names.
c. No. of drugs from National Essential Drug List of Pakistan12.
d. No. of injectable preparations.
e. No. of antimicrobials.
f. Approximate cost of the prescription (per day).
g. Whether the diagnosis is listed on the prescription.
h. Relevance of the treatment prescribed to the diagnosis.
i. Whether the dosage of the drugs prescribed is appropriate.
j. Whether the advised duration of the treatment is appropriate. Final analysis of the data obtained from individual
prescriptions was carried out on computer using statistical software, Epiinfo.
Results
A total of 601 prescriptions were studied, whose distribution in relation to various disciplines is given in Table I.
Seventeen hundred and eighty three drugs were prescribed in these prescriptions. The mean number of drugs per prescription was 2.97 with a range of ito 9 drugs in outdoors and ito 12 drugs in indoors. Data of individual departments is shown in Table II.
The essential drugs, as laid down in the National Essential Drug List of Pakistan, constituted 80.3% of the total drugs prescribed. Only 23.6% drugs were prescribed by their generic names (Table III).
Injectable proportions were 17. 1%of the total drugs prescribe, being most frequently used in the indoor paediatric patients (53.5%). Antimicrobials were 20.4%, upto 7 drugs being encountered ma single prescription (Table IV).
The average cost of treatment per day was Rupees 26.10 in outdoor and Rs.88.36 in indoor departments. However, an extremely wide variation in the cost of treatment was found, as depicted in Table V.
Diagnosis was mentioned on 83.0% of the studied prescriptions while it was omitted in the remaining 17%. The treatment prescribed was found to be relevant to the diagnosis given on the prescription in 55.9% cases while it was partially relevant in another 19.5% prescriptions. The treatment apparently did not correlate to the diagnosis in 24.6% of the prescriptions (Table VI).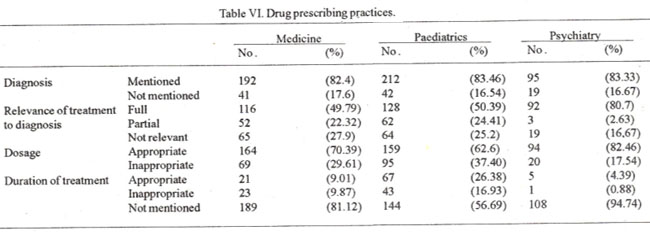
The drugs were administered inappropriate doses in 69.4% cases while an apparently inappropriate dosage was noticed in the remaining 30.6% prescriptions (Table VI). Duration of treatment was not specified on 73.4% prescriptions. Of the remaining 26.6%, the duration was appropriate in 15.5% and inappropriate in 11% cases (Table VI).
Discussion
The overall average number of drugs per prescription found in this study is 2.97. The number was higher in indoor (3.27) as compared to the outdoor prescriptions (2.42), the highest average being encountered in the medical indoor departments i.e., 4.01 drugs per prescription. The figure found in this study is comparable to that reported from Kenya13 and Democratic Yemen where an average of 3 drugs per prescription are prescribed. However, it is far from ideal and higher as compared to the developed countries like Switzerland where an average of only 2 drugs perprescription have been reported14. A tendency towards polypharmacy was noticeable in several individual prescriptions studied by us; as many as 9 and 12 drugs were encountered in single prescriptions from outdoors and indoors respectively. This indicates a room for improvement as polypharmacy is attended with the risk of drug toxicity, reduced patient’s compliance, higher cost of treatment and greater chances of drug interactions. It was interesting to note that in one prescription from an indoor medical unit, the treatment solely comprised of non- pharmacological measures. We feel that this practice needs to be promoted in mild cases of diabetes mellitus, hypertension. obesity and hyperlipidemias. It was encouraging to note that essential drugs, as defined by the Ministiy of Health in the National Essential Drug List of Pakistan, are being given due importance in therapeutic practice and over 80% of the prescribed drugs belonged to this category. The concept of essential drugs has proved extremely useful in satisfying the health care needs of the masses. The selection of the essential drugs is however, a continuing process that should take into account the changing epidemiological conditions as well as the progress in the pharmacological and pharmaceutical knowledge. It should also be accompanied by a concomitant effort in education and training of health personnel in use of the drugs9.
The use of generic preparations was found to be not much in vogue. Only 23.6 1% of the total drugs were prescribed by their generic names. This may be largely due to non-availability of most of the drugs in generic preparations. Further, the prescribers also have reservations about the quality of generic preparations. It was observed that in institutions where hospital formularies are based on genetic preparations of essential drugs, the hospital staff is also inclined to prescribe in a similar fashion. The hospital fonnularies therefore, can play an important role in determining and modifying the prescribing pattern in an institution15.
Injectable preparations of the drugs were used in 17.1% cases. Their use was relatively more frequent in the admitted patients which correlates with the severity of illness in this group. Highest incidence of use of of injectables was noticed in the indoor pediatric departments where injectables outclassed the oral dosage forms (53.5% vs 46.5%). Whereas it was difficult to adjudge the rationality of the use of injectables just by reviewing the prescribing record. Certain discrepancies were obvious. For example in one of the gastroenterology units, injection Flagyl (metromdazole) was used veiy frequntly , in some case even without evidence of a judicious indication. Metronidazole has asmailmolecularsize and is highly li?id soluble. Oral bioavailability of the drug is more than 99%16. Oral administration of the drug is therefore, effective even in deep seated infections. Injectable form of metronidazole is also not cost-effective17. Antimicrobials were used in 20.45 of the cases with a wide variety of drug choices ranging from first line drugs like penicillins and erythromycin to fluoroquinolones and third generation cephalosporins. Combinations of antimicrobials were also frequently seen and as many as 7 drugs were encountered in one prescription. Antimicrobials were invariably prescribed to the cases of acute respiratory infections (ARI) and gastroenteritis. In a recent study more than 97% cases of AR! from Rawalpindi/Islamabad area were found to be viral in origin, thus not requiring antibiotic therapy. There is a strong association between the magnitude of antimicrobial use and the emergence and spread of resistant strains of bacteria18. Itis therefore, a timely requirement to rationalize the use of antimicrobials in our society.
A wide variation in the cost of treatment was observed, the average per day cost being Rs.26. 10 in the outdoor and Rs.88.36 in the indoor departments. Treatment cost as high as Rs. 1871 per day was noticed in an individual prescription. Polypharmacy, use of injectables and choice of branded costly drugs recently introduced in the market with doubtful claims of superiority over the older cheaper alternate drugs were the main factors contributing towards the high cost of treatment. Cost should be considered one of the important factors in making a therapeutic decision. In developing countries with limited financial resources, a rigorous economic approach is required to provide the minimum essential health facilities to the masses19.
Diagnosis was listed on more than 83% prescriptions. It was mostly in the outdoor prescriptions where an omission of diagnosis was encountered. This may be due the heavy work-load of the doctors in the outdoor departments of the government hospitals.
It was difficult to adjudge the relevance of the treatment to the diagnosis due to various reasons. In several cases drugs were prescribed for the symptoms unrelated to the diagnosis. In some prescriptions it appeared as if some intercurent illness had arisen the need for additional treatment that was unrelated to the recorded diagnosis. With such limitations, it was possible to study only the apparent correlation between the treatment prescribe and the diagnosis listed on the prescription. On the whole such correlation was fully established in 55.9% cases.In 19.5% cases a partial relevance was observed, while in the remaining 24.6% prescriptions a correlation between the treatment and diagnosis was completely lacking. This figure, although alarming, is comparable to that reported from USA where 20 to 40% prescriptions were found to be irrelevant to the diagnosis5,6.
The dosage apparently appeared to be inappropriate in 30.6% cases. However, dose of drug is determined by a host of factors20 that cannot be studied merely by reviewing the prescription. Duration of the treatment was appropriately specified only on 15.5% prescriptions. It was inappropriate in 11.2% cases while in the remaining 73.4% prescriptions the duration of treatment was not specified at all. The correct duration of treatment is an important determinant of successful therapy and must be communicated to the patient and paramedical staff responsible for administration of the drugs. Itis particularly important incase of psychotropic drugs and antimicrobials to avoid the problems of drug-dependence and drug-resistance. We conclude that appropriate educational, managerial and regulatoiy interventions may be evolved to rationalize the drug use in Pakistan. Educational outreach through printed materials and face to face discussions with the prescribers has been shown to improve the drug-use decisions, the latter approach being more effective thanthe former21. Sucheducationcanbe imparted as apart of in-service training of the doctors. Managerial strategies canalso help to promote rational use ofdrugs. These may include strict procedures for selection and procurement of drugs, development and dissemination of treatment guidelines for selected diseases and pricing of drugs according to their health impact. Inaddition, apowerful mechanism needs to be developed tolimitthe number of available drugs through regulatory control.
Acknowledgements
The authors express their gratitude to Dr. Khalid Saeed, Dr. G.R. Mashori, Miss Bushra Tayyaba Khan and Mr. A.Q. Javed for their help and assistance incollectionand analysis of the prescriptions.
References
1. Hogerzeil, H.V. Promoting rational prescribing: An international perspective. Br. S. Clin. Pharmacol., 1995;39:l-6.
2. Lapotte, JR., Baksaas, I. and Lunde, P.K.M. General background. In: Drug Utilization studies: Methods and uses. Dukes, MNG. (ed). Copenhagen, WHO Regional Office, 1993, pp. 5-22.
3. Stanulovic, M., Kakovijevic, V and Roncevic, N. Drug utilizaion in paediatrics: Non-medical factors affecting decision making by prescribers. Eur. S. Clin. Pharmacol., 1984;27:237-241.
4. Tognoni, G. and Laporte, JR. From clinical trials to drug utilization studies. In: Drug utilization studies: Methods and uses. Dukes. M.N.G. (ed). Copenhagen, WHO Regional office for Europe, 1993, pp. 23-41.
5. Palombo, F.B., Knapp, D.A. Erandon, B.M. et al. Detecting prescribing problems through drug usage review: A case study. Am. J. Hosp. Pharm., 1 977;34: 152-54.
6. Maki, DO. and Schuna, A.A. A study of antimicrobial misuses in a university hospital. Am. J. Med. Sci., 1978;275:271-282.
7. Baksaas, 1. and LUnde, P.K.M. National drug policies: the need for drug utilization studies. Trends Pharmacol., Sci., 1 986;7:23 1-234.
8. WHO Expert Committee, The selection of essential drugs. (Technical Report Series 615). Geneva, WHO, 1977.
9. WHO Expert Committee, The use of essential drugs. (Technical Report Series 770). Geneva, WHO, 1 988.
10. Ali, H.M. Problems in assessing rationality of drug utilization in less developed countries. Acts Med. Scand., 1986,721(Suppl):27-30.
11. World Health Organization. Selected drug use indicators.ln: How to investigate drug use in health facilities. Action Programme on EssentiaIDrugs. Geneva, WHO, 1993.
12. National essential drug list of Pakistan. Sheikh, N.M. (ed). Islamabad Ministry of Health, Government ofPakistan, 1994.
13. Maitai, C.K. and Watkins, W.M. A survey of outpatient prescriptions prescribed in Keny atta National Hospital. East Afr. Med. J., 1980;57:641 -645.
14. Hogerzeil, H.V. Strategies to promote rational drug use. Action Programme on Essential Drugs and Vaccines, Geneva, World Health Organization, 1995.
15. Abramowitz, P.W. Controlling financial variables - changing prescribing pattersn. Am. J. Hosp. Pharm., 1984;41 :503-5 15.
16. Leslie, T. and Webster, Jr. Drugs used in chemotherapy of protozoal infections: Amebiasis, giardiasis and trichomuniasis. In: The pharmacological basis of therapeutics. Gilman, AG,, Rall, TW. et al. (eds). New York, USA, Pergarnon Press,lnc., 1991, pp. 999-1007.
17. Akhtar, M.A. Antimicrobial treatment. In: Rational therapeutics: A costeffectie approach. Islambad, Printing, Packaging and Paper converting Corporation, 1991,pp. 36-51.
18. McCaig, L.F. and Hughes, 3M. Trends in antimicrobial drug prescribing among office-based physicians in United States. JAMA., 1995;273 :2 14-2 19.
19. Akhtar, MA. and Najmi,M.H. Guidelines for rational use of drugs. Pak. Armed Forces Med. J., I 992;42:52-54.
20. Cheema, M., Khan, A. and Yusuf, SM. Oneeral pharmacology. In: Multiauthor Textbook of Pharmacology and Therapeutics. Lahore, Pakistan, National Medical Publications, 1992, pp. 1-100.
21. Avorn, J. and Soumerai, S.B. Improving drug-therapy decisions through educational outreach. N. Engi. J. Med., 1983;308: 1457- 1463.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: