
Zeba Hasan Hafeez ( Department of Dermatology, Dow Medical College and Civil Hospital, Karachi. )
February 1998, Volume 48, Issue 2
Review Articles
The association offoods with atopic dermatitis, urticaria and dennatitis herpetiformis has been known for a long time. “Food allergy” has become a fashionable diagnosis although its basis may be insubstantial. Ingested allergens undoubtedly play a role in the symptoms of some atopic patients and gastrointestinal signs suchas lip swelling, vomiting, diarrhoea and pmritus ani may be associated as well1. Salicylates and food additives particularly colours could alter children’s behaviour and development2. Food intolerant children have been found to be 1.5 cm shorter than normal children3.
Atopic eczema
Food allergy/intolerance may trigger atopic dermatitis (AD) in a small subgmup of patients and is more commonly implicated in children than in adults . The Radio allergosothent tests (RAST) and skin-prick tests have given a further stimulus to dietary factors in this disease. Food appears to be more important than food additives when diet is involved inthe worsening of eczema. Food intolerance exists in 0.3% to 20% of children5. Although 20% of parents suspect their children (under 6 years) to have food related illness, only 20% to 30% of these will have this confirmed by appropriate challenge and the tme figure for food intolerance could be around 5%6 . In 1992, a study confirmed the relation between food allergy and atopic disease in 250 children with AD. Ninety-six percent of all children with severe AD had food sensitivity. The most commonly implicated foods were eggs, cow’s milk, fish, shellfish, corn starch, peanuts and soybeans. Food sensitivity persisted in 67% of children with severe atopic dermatitis upto 7 to 15 years of.age and was always associated with aero-allergen sensitivity - Type I food allergy occurs predominantly in those patients with AD who have a predisposition to respiratory atopy. RASTs performed in 183 patients with AD showed that about half of them had type I allergy to atleast one of the five common foods. The RAST correlated roughly to the severity of dermatitis. In each group of patients with mild, moderate and severe AD, positive RAST reactions to common foods occured mainly in patients who had a personal orfamily8history of respiratory atopy and were rare in cases of pure AD Food intolerance has been frequently observed in AD patietns with high IgE levels9. In another study, IgE binding components of wheat, rye and oats were recognized by immunoblotting analysis with sen from adults with AD10 Immediate hypersensitivity to bakery, brewery and wine products (beer, aged red wine, young and sparkling white wine and extracts of fresh wheat bread and dried rye bread) in yeast sensitive patients has also been described11. Rice allergy was noted in severe AD in Japan, the clinical severity of which was closely related to the semm IgE values and RAST positivity12. Colourings and preservatives have been implicated in some children13 - Food allergies often subside with age14,15. Allergy to cows milk was recognized in ancient Greece and the familial nature of astluna was ttported by Maimonides in 1100 AD2. Cow’s milk intolerance affects up to 7.5% of young children, but 80% of these are expected to get over their intolerance by the age of 3 years. Egg and wheat intolerance is transient in children, but allergy to fish/shellfish, peanuts and tme nut is persistant2.
Management
Food allergy/intolerance should be considered in the management ofAD when there is a history of provocation with food or when conventional treatment is ineffective or both. Positive skin tests to eggs, milk, peanuts, fish, soy, wheat and shelffish should be followed by withdrawal of foods responsible for AD. On improvement after withdrawal of one or two foods, continued avoidance is advised. If several foods are involved, double-blind, placebo-controlled food challenges can be performed in an attempt to reintroduce the foods. Maternal and infant allergen avoidance is beneficial in infants at high risk of àtopy (atopy in both parents, one parent and sibling, two siblings, first degree relatives and elevated cord IgE levels)16. A genetically predisposed infant is less likely to develop atopic symptoms if purely breast-fed. Breast milk contains a high concentration of IgA, offering a protective role, but may contain maternally ingested allergens. Therefore, maternal diet should exclude major allergens while breast feeding and during late pregnancy as sensitization is said to occur in utero17. The beneficial effects of maternal and infant allergen avoidence were not sustained at 7 years of age. Mothers in the avoidance group avoided cow’s milk until one year, eggs until 2 years, peanuts and fish until 3 years. There was a significant reduction in food allergy and milk sensitization before two years but no difference between groups at 7 years regarding food or aero-allergen allergy, AD or asthma18. If foods are excluded from the diet in infancy, no attempt should be made to reintroudce them before the age of 12 months after which supervised reintroduction of milk, wheat and eggs should be considered at 6 monthly intervals. This should be done in a hospital setting if adverse reactions are anticipated. In severe cases of AD who have failed to respond to general and topical therapy, a 3-4 week trial period of avoidance of beef, eggs, chicken, food additives and nuts should be tried. Suspected foods can be introduced one at a time every 37 days19. Sodium cromoglycate has not been found useful in the management of food allergy and as yet, the only effective treatment is complete avoidance of the offending food. However, there are compliance problems in the dietary management of disease with resultant relapse of atopic eczema as the diets may impose an immense financial and emotional burden on children and parents. Even in highly motivated parents of children with severe manifestations of food intolerance, diets would be difficult to maintain in 20% of children under 3 years and upto 50% of those over 3 years. Many patients and their parents have indicated that the diets are worse than the disease13.
Urticaria/Angioedema
Urticaria/angioedema affects approximately 15% of the population at sometime in their lives20. Urticaria may occur alone in about 40%, as angioedema in approximately 11% and both in 49% of patients21. Urticaria is described as chronic if it persists for more than three months. Despite exhaustive investigations an etiological cause is found in fewer than 20% of patients. Complete blood counts, ESR, food diary and a trial of additive- free diet are the appropriate routine investigations22. In Pakistan, serial stool examinations should be done to exclude protozoal and worm infestations. Urticarial reactions to tartrazine in drugs were first described in 195923. Ina study of330 patients with chronic urticaria, one-third were aggravatedby food additives24 and in another 24 of49 patients improved with an additive-free diet25. The additives most commonly implicated are the azo dyes tartrazine, amaranth, sunset yellow and carmoisine. Annatoo a natural carotenoid dye used as an additive to colour dairy products and cheese, is also a suspect26. The benzoate preservatives and antioxidants butylated hydroxytoluene (BHT) and butylated hydroxyamsole (BHA) are incrimminated less often than colours.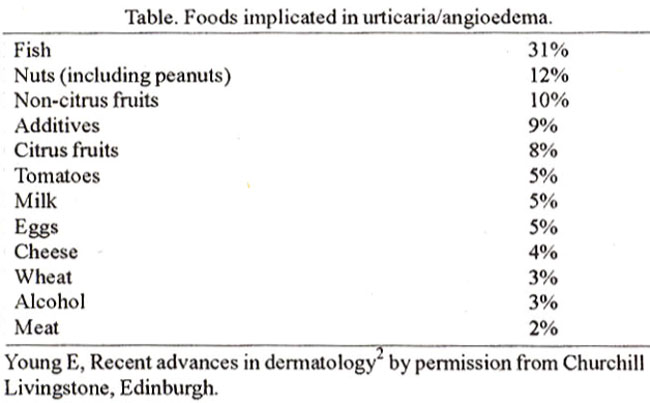
The frequency of aspirin intolerance by history in 2,592 normal individuals was 0.3%, and it was over 20 times greater in those with recurrent urticana than in normal individuals (3.8% v/s 0.3, P less than 0.001)27. Salicylates occur in the natural foods as sodium salicylate in low levels. Salicylates are present in many fruits (e.g. apples, bananas), wine, vinegar, liquorice and as an additive in jam, jelly, icecream, chewing gum and soft drinks. An appropriate exclusion diet has been found beneficial in salicylate sensitization urticaria and angioedema1. Cross sensitivity between aspirin, tartrazine and other azo dyes is common. In 131 patients with chronic urticaria including physical urticaria, oral provocation tests were done with aspirin. Reactions wre seen in 35% of patients with idiopathic urticaria, 52% with cholinergic urticaria and 43% of those with pressure urticaria28. There is a controversy about the mechanism of allergy in tartrazine sensitivity, whether it is immunological29 or pharmacological30 in nature, as appears to be the case with aspirin sensitivity31 (cyclo-oxygenase inhibition with interference of the prostaglandin pathway)32.
Acute and childhood urticarias usually have a food related aetiology as compared with chronic urticaria where there is a low incidence of food allergy. Most acute food related urticarial reactions occuring in atopics are IgE mediated but canbe secondary to the histamine contentof food e.g. scromboid fish, tuna, mackerel33, strawberries and egg white. IgE mediated urticaria in atopics may cause immediate itching, tingling and swelling of the lips. The ingested food may be vomited and if enough is absorbed generalized urticaria and even anaphylaxis can occur. Milk, nuts and fish may also cause allergic contact urticaria affecting the lips, face and fingers. Delayed pressure urticaria has been associated with ingestion of chocolates and peanuts in one study34. Urticaria/angioedema and anaphylaxis have been reported on ingestion of a food but only after exercise29,35. This well recognised syndrome has been reported with shellfish, nuts and celery2. Penicillin related urticaria can be induced by milk containing penicillin in sensitive subjects36, and when present inbeef, frozen meals and soft drinks. Chronic urticana has also been reported with nickel intake as judged from type I and IV sensitization to nickel positive oral challenge test and long standing complete remission with a nickel restrictive diet37.
Dermatitis due to nickel content in diet Nickel sensitive patients may experience persistent dermatitis even if they avoid cutaneous contact with nickel plated items. In one study, 90 nickel-sensitive patients who had a flare of dermatitis after oral challenge with 2.5 mg nickel but no reaction to placebo were instructed to adhere to a low nickel diet. Fifty-eight of the 90 patients benefitted in the short term nickel free diet. In this study it was observed that psychologic stress also caused flares38. Various foods and drinks can aggravate nickel dermatitis even though their nickel content may be low. These include beer, wine (particularly red wine), herring, tuna, tomatoes, onions, carrots, apples and citrus furits. The first litre of water from the tap should be discarded in the morning as nickel may be released from the tap at night. Nickel plated kitchen utensils should be replaced and acid foods such as stewed fruits cooked in stainless utensils should be avoided. Canned food should be eaten in moderation. Nickel cannot be completely eliminated from the diet as many foods have a low nickel content. The following items have a high nickel content and canbe avoided. Shellfish like shrimp, mussels and crawfish, tea from drink dispensers, chocolate milk, beans and bean sprouts, kale, leeks, lettuce, lentils, peas, soy protein powder, spinach, bran, buckwheat, millet, muesli and similar breakfast cereals. Multigrain breads, oatmeals, rice (unpolished), rye bran, sesame and sunflower seeds. Dates, figs, pineapple, prunes and raspberries. Almonds, baking powder (in large amounts), hazelnuts, peanuts, sweets containing marzipan, strong licorice and vitamins containing nicke13
Conclusion
Food and food additive reactions are frequently proposed by patients as a cause of their dermatological complaints. Although most of these are false impressions, they should not be ignored and a detailed history, diet-diary and trialof food eliminationforfourweeks may be tried. With no clinical improvement, reassurance is advised. However, if there is improvement double- blind, placebo-controlled challenge provides the correct diagnosis. Skin-prick testing and RAST estimation are not sufficiently accurate for diagnostic purposes. Food challenge should be medically supervised and due caution should be &ercised if severe reactions are expected. When children are put on elimination diets and where major foods are involved referral to a specialist centre and a dietitian’s supervision is mandatory.
References
1. Jackson, W.F. and Certo, RA. A Colour Atlas of Allergy. London, Wolfe Medical Publications, 1988, pp. 88, 91.
2. Young, E. Food additives, food and dermatology. Recent Advances in Dermatology, No. 9. Ed. Champion, RH. and Pye, R.J London, Churchill Living stone, 1992. 133-145.
3. Price, C.E., Rons, R.J. and Chinn, S. Height of primary school children and parents: Perceptions of food intolerance. Br. Med. J., 1988;296:1696-1699.
4. Rothe, M.J. and Orsnt-Kels, J.M. Atopic dermatitis: An update. J. Am. Acsd. Dermstol., 1996;35:1-13.
5. Ogle, K.A. and Bullock, J.D. Children with allergic rhinitis and/or bronchial asthma treated with elimination diet. Ann. Allergy, 1 977;39 :8-11.
6. Sampson, HA. Immunologically mediated food allergy: The importance of food challenge procedures. Ann. Allergy, 1988;60:262-269.
7. Guillet, G. and Guillet, M.H. Natural history ofsensitization in atopic dermatitis: A three year follow-up in 250 children. Arch, Dermatol., 1992;! 28:187-92.
8. Uehsrs, M., Kimura, C. and Uenishi, T. Type 1 allergy to food in atopic dermatitis. Comparison between RAST - positive and RAST- negative cases. Acts Derm. Venereol., Suppl. (Stockh), 1992;176:38-40.
9. Rudzki, E., Samochocki, Z., Rebandel, Petal. Frequency andsignificsnceofthe major and minor features of Hanifin and Rsjks among patients with stopic dermatitis. Dermatology, 1994;189:40-6 6.
10. varjonen, E., Savolainen, J., Mattila, L. et al IgE binding components of wheat, rye, barley and oats recognised by immunoblotting analysis with sera from adult atopic dermatitis patients Clin. Exp. Allergy, 1994;24:481-9.
11. Kortekangas, S.O., Savolainen, J., Lantto, R. et a!. Immediate hypersensitivity to bskery, brewery and urine products in yeast sensitive stopic dermatitis patients. Clin. Exp. Allergy, 1994;24:836-42.
12. tkezawa, Z., Miyakawa, K., Komatsu, H. et al A probable involvement of rice allergy in severc type ofatopic dermatitis in Japan. Acts Derm. Venereol. Suppl. Stockh 1992; 176:103-7.
13. Hathaway, M.J and Wsrner, JO Compliance problems in the dietary management of eczema. Arch. Dis. Child, 1 983;5 8:463-464.
14. Dannseus, A. and Inganas, M. A follow up ofchildren with food allergy. Clinical course in relation to serum IgE and IgG antibody levels to milk, egg and fish. Clin. Allergy, 1982;11 :533-9.
15. Ford, R.P.K. and Taylor, B. Natural history of egg hypersensitivity. Arch. Dis. Child., 1 982;57:649-52.
16. Hide, D.W., Matthaews, S., Matthews, L. et al. Effects of allergen avoidence in infancy on allergic manifestations at age two years. J. Allergy Clin. Immunol., 1994;93:842-6.
17. Zieger, R.S., Heller, S.,MeIlon,M. etal. Effects ofcombined matemaland infant food allergen avoidence on development of stopy in early infancy. 2. Allergy Clin. Immunol., 1989;84:72-84.
18. Zeiger, RS. and Heller, S. The development and prediction of atopy in high risk children: Follow-up at age seven years in a prospective randomized study of combined maternal and infant food allergen avoidence. J. Allergy Clin. Immunol., l995;95:l 179-90.
19. Champion, RH. and Parish, WE. Atopic dermatitis, In: TextBook ofDermatology. Rook, Wilkinson, Ebling,Ed. Champion,R.H., Burton, J.L. and Ebling, F.J.G., Fifth S., London, Blackwell Scientific Publications, 1992, pp. 608, 1879.
20. Sheldon, J.M., Matthews, K.P and Love!!, R. G. Thevexing urticaria problem. 2. Allergy, 1 954;25:525-527.
21. Champion, R., Roberts, S., Carpenter, R. et al. Urticaria and angioedema: A review of 554 patients. Br. 2. Dermatol., 1 969;8 1:588-597.
22. Black, AK., Greaves, MW., Champion, R.H. et al. The urticarias 1990: A report of a meeting. Br. 2. Dermatol., 1991; 124:100-108.
23. Lockey, S.D. Allergic reaction due to F D and C yellow No.5 Tartrazine, an aniline used as a colouring and identifying agent in various steroids. Ann. Allergy, 1959;17:719-721.
24. Juhlin, L. Recurrent urticaria: Clinical investigation of 330 patients. Br. 2. Dermatol., 1981;104:369-381.
25. Murdoch, RD., Pollock, I. and Naecm, S. Tartrazine induced histamine release invivo in normal subjects. JR. Coil, Physicians, 1987a;21:262-266.
26. Mikkelsen, H., Larsen, J.C. and Tarding, F. Hypersensitivity reactions to food colours with special reference to the natural colour annatto extract. Arch. Toxieol., 1978; Suppl I: 141-143.
27. Settipane, R., Constantine, H.P. and Settipane, G.A. Aspirin intolerance and reeurrenturtiearis in normal adults and children. Allergy, 1980;35:149-154.
28. Doeglas, H.M. Reactions to aspirin and food additives in patients with chronic urticaria including the physical urticariaa. Br. 2. Dermatol., I 975;93: 135-44.
29. Weliky, N. and Iteiner, C. Hypersensitivity to chemicals, correlation of tsrtrazine hypersensitivity with characteristic serum IgD and IgE immune response pattems. Ciin. Allergy, 1980; 10:375-393.
30. Murdoch, R.D., Pollock, I. and Young, E. Food-additive induced urticaria: Studies of mediator release during provocation tests. 2. R. Coil. Physicians, 1987b,21:262-266.
31. Asad, S.L, Youiten, L.J.F and Less of, M.H. Specific desensitization in aspirin-sensitive urtiesria: Plasma prostaglandin levels and clinical manifestations. Clin. Allergy, 1983; 13:459-466.
32. Williams, W.R., Pawlowiez, A. and Davies, B.H. Aspirin-likeeffeetsofselected food additives and industrial sensitizing agents. Clin. Exp. Allergy, 1989;19:533-7.
33. Taylor, SI. Histamine food poisoning: Toxicology and clinical aspects. CRC. Cri. Rev. Toxieol., 1986;l7:91-l28.
34. Davis, K.C., Mekori, Y.A., Kohler, PR eta!. Possible role of diet in delayed pressure urtiearia: Preliminary report. J. Allergy Clin., Irnmunol., 1986;77:566-569.
35. McNeil, D. and Strauss, R. Exercise-induced snaphylaxis related to food intake. Ann. Allergy, 1988;64:440-442.
36. Ormerod, A.D., Reid, TM.S. and Main, R.A. Penicillin in milk: its importance in urtiearia. Clin. Allergy, 1 987;1 7:229-234.
37. Abeek, D., Traenekner, I., Steinkras, V. et a!. Chronic urtiearia due to nickel intake. Acts Derm. Venereol., 1993;73:438-9.
38. Vein, N.K., Hattel, t. and Laurberg, G. Low nickel diet: An open, prospective trial. JAm. Dermatol., 1993;29:1002-7.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: