
Muhammad Ali ( Department of Cardiology, Tabba Heart Institute, Karachi, Pakistan. )
Faisal Qadir ( Department of Cardiology, Tabba Heart Institute, Karachi, Pakistan. )
Salman Javed ( Medical Students, Dow Medical College, Dow University of Health Sciences, Karachi, Pakistan. )
Zohaib Nawaz Khan ( Medical Students, Dow Medical College, Dow University of Health Sciences, Karachi, Pakistan. )
Sidra Asad ( Medical Students, Dow Medical College, Dow University of Health Sciences, Karachi, Pakistan. )
Bashir Hanif ( Department of Cardiology, Tabba Heart Institute, Karachi, Pakistan. )
April 2012, Volume 62, Issue 4
Original Article
Abstract
Objective: To determine factors affecting cardiac rehabilitation attendance after myocardial infarction and coronary revascularization.
Methods: A cross-sectional study was conducted on 416 patients admitted in Tabba Heart Institute, Karachi from December 2010 to May 2011. Patients admitted with diagnosis of acute myocardial infarction (AMI) or who underwent elective coronary artery bypass graft surgery (CABG) or percutaneous coronary intervention (PCI) procedures were offered cardiac rehabilitation (CR). Out of these, patients who enrolled in 6 weeks outpatient CR programme were followed for number of CR sessions and their socio-demographic and clinical data were collected. Data was analyzed by Statistical Package for Social Sciences (SPSS) software, version 15.0. Chi-square test was applied to test association between categorical variables and Student\\\'s t-test for continuous variables.
Results: Out of 416 patients identified, only 151 patients (36.2%) enrolled and attended the CR programme. Of the 151 attendees, 111 (73.4%) patients subsequently completed more than 6 weeks of outpatient CR programme. We found significant association between CR attendance and easy access to the programme, elective CABG procedure, employment status, presence of diabetes or hypertension and baseline level of exercise (all p < 0.01). No association was found between CR attendance and patient age, gender, body mass index or different economic groups.
Conclusion: Attendance rates of patients attending outpatient CR programme after AMI or coronary revascularization procedures are suboptimal. Patients who underwent elective CABG surgery and had easy access to the CR programme had better attendance. Factors contributing to poor attendance rates at CR programmes in developing countries need to be explored and subsequently addressed.
Keywords: Myocardial infarction, Coronary revascularization, Chi-square test, Karachi (JPMA 62: 347; 2012).
Introduction
Cardiac rehabilitation (CR) refers to a secondary prevention, medically supervised programme, designed to enhance physical, psychological and social functioning of patients with heart disease.1 CR comprises of low-to moderate-intensity, supervised physical activity but also patient counseling and education regarding control of risk factors contributing to cardiovascular disease (CVD). It is usually initiated 1 to 3 weeks after a cardiac illness and is an important measure in enabling patients to return to active life early.2 CR initially designed for inpatients, has undergone tremendous modifications over the years and is now a completely integrated outpatient programme. The advantage to patients undergoing formal CR sessions after cardiac illness is multifold. CR has also been proven to play a major role in reducing the rate of major adverse cardiac events (MACE) in revascularised patients.3,4
Despite its usefulness, global attendance rates at CR programmes are low. In our part of the world, it is not a surprise that there are only a handful of centres that offer supervised cardiac rehabilitation services to patients recovering after a cardiac illness. There are a number of obstacles leading to poor attendance at CR centres; these include patient\\\'s refusal to make any lifestyle changes, poor referral system, lack of adequate CR programmes, and socio-economic issues particularly lack of insurance coverage. The American Heart Association emphasizes the need to identify patients who would most likely benefit from CR and also focus on their medical and social profiles to obtain maximum benefit and prevent drop-outs from the CR programmes.2
Modern CR programmes usually comprise of three phases: inpatient rehabilitation (Phase 1), outpatient rehabilitation (Phase 2) and maintenance phase (Phase 3 and 4).5 The main focus of our study was the outpatient CR service, since it is this component of CR that has been most widely and extensively documented to impart benefit to its participants. We selected patients who suffered an acute myocardial infarction and received thrombolytic therapy and also patients who underwent elective coronary revascularization procedures and assessed their attendance rates at an outpatient CR programme. We also observed the association of medical and socio-demographic factors on the CR attendance.
Patients and Methods
All consecutive patients admitted with the diagnosis of acute myocardial infarction (who received thrombolytic therapy or subsequently underwent in hospital coronary revascularization- PCI or CABG) and patients undergoing elective CABG or PCI, at the Tabba Heart Institute Karachi during the period December 2010 to May 2011 were identified (Figure). Of these, patients who subsequently registered at our outpatient CR programme were included in the study. Patients with severe functional impairment (neurological, cognitive or joint disease) or coexisting debilitating co-morbidities hindering in participation at CR sessions were excluded from this study.
A questionnaire was designed to assess clinical, demographic and socio-economic factors affecting the attendance rates. Factors included patient age, gender, body mass index (BMI), clinical diagnosis or procedure, co morbid conditions, economic groups, access to cardiac rehabilitation programme and baseline level of exercise. The economic groups were divided in accordance with the World Bank Data, based on approximate yearly income into low (less than $ 996 /year), middle (between $ 996 - 12195 /year) and high income groups (greater than $ 12195 /year). Easy access to CR programme was defined as patients having personal conveyance and living nearby within 15 km vicinity to the Rehabilitation center. Baseline level of exercise was categorized as low level - less than 5 walking sessions/ week or high level- greater than 5 walking sessions/week. The socio-demographic factors were gathered either from the medical record or directly from the patient. The patients enrolled were tracked for the number of sessions attended, by reviewing the files every week with the cardiac rehabilitation coordinator.
Collected data was entered and analyzed by the Statistical Package for Social Sciences version 15.0 Software (SPSS Inc., Chicago, Illinois). Continuous variables such as age and BMI were expressed as mean ± SD and categorical variables were presented as frequencies and percentages.
Chi-square test was used to evaluate the relation between categorical variables and Student\\\'s \\\'t\\\' test for continuous variables. All significance tests were two tailed and the results were considered statistically significant when the p value < 0.05.
Results
Out of a total of 2560 patients who were consecutively admitted in the hospital with various clinical diagnoses , 416 patients were found eligible to be enrolled in the study based on admission diagnosis of acute MI or elective PCI or CABG surgery. These patients were offered outpatient cardiac rehabilitation and were followed for attendance in CR sessions (Figure).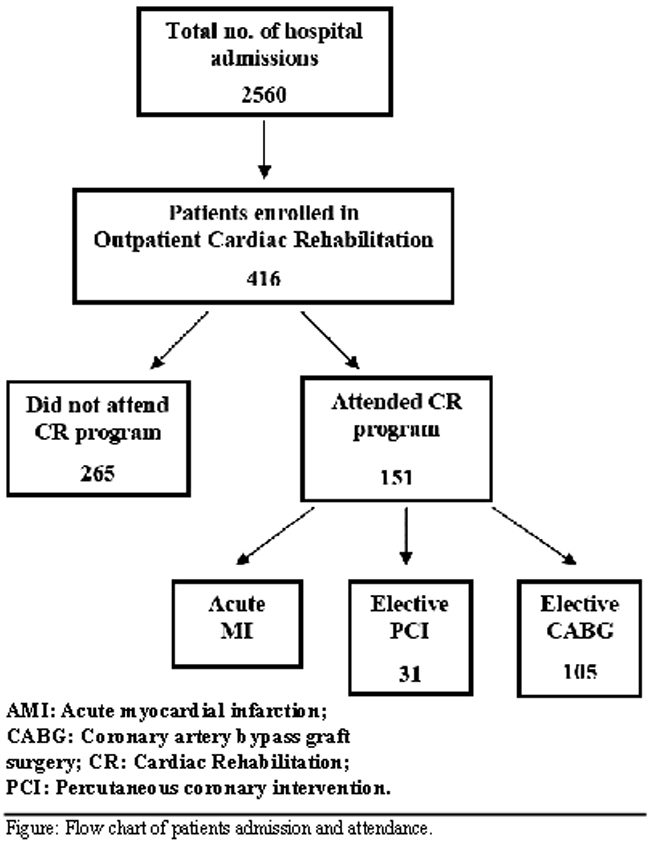
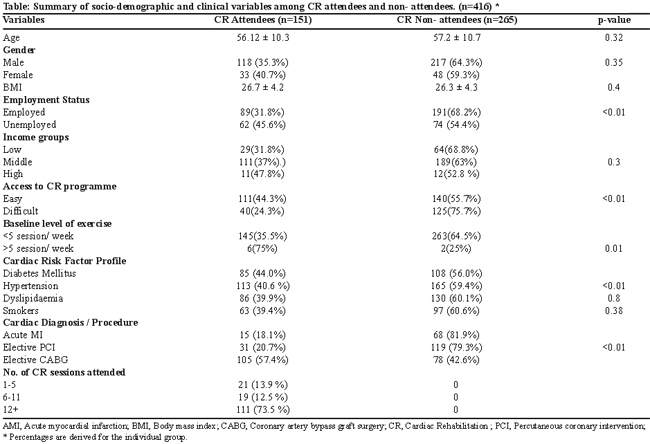
Table illustrates the frequencies of variables including socio-demographics, cardiac risk factor profile and cardiac diagnoses among the attendees and non-attendees. Only 36.3% patients finally attended the outpatient CR programme. Among the CR attendees, there were 78.1% male and 21.9% female patients. There was no association between CR attendees and non-attendees in terms of age, gender and BMI status. Out of 83 patients in the study group who had acute MI, only 18% patients attended outpatient CR (p < 0.01). On the other hand out of 150 patients who underwent elective PCI, 20.7% attended CR (p < 0.01), while from the elective CABG surgery group of 183 patients, 57.4% attended CR (p < 0.01). The results highlight that attendance rate was higher for patients undergoing elective coronary revascularization procedures (PCI / CABG) 90%, as compared to patients having acute MI 10% (p?0.01).
Access to the CR programme was also a major factor contributing to CR attendance. Patients having easy access to the programme had better attendance (44.2%) than those having difficult access (23.9%), p < 0.01. Patients who were currently employed had lower attendance rates (31.7%) as compared to patients who were unemployed, (45.6%), p < 0.01. The income status of the patients had no significant association with attendance rates.
In the overall study group of 416, only 8 patients had a baseline level of exercise > 5 walking sessions per week before AMI or coronary revascularization procedure. Hence forth, comparison cannot be determined among the attendees and non attendees in terms of the influence of baseline level of exercise on attendance rate.
The results showed that only 40 patients out of the 151 patients, who joined the programme, did not attend 6 weeks of outpatient CR sessions, which shows a drop out rate of 26.5% (p < 0.01).
Discussion
In developing countries, formal and structured outpatient cardiac rehabilitation programmes are extremely limited. Moreover, the attendance rate of patients attending such programmes after a cardiac illness or cardiac procedure is suboptimal. The results of our study highlight this aspect with only a third attending CR sessions. This is similar to the rates seen in the study by Cooper et al. In their review of 18 international studies from USA and UK, the average attendance rate at outpatient CR was 43%.6 The Healthcare Commission in UK also reported that, in 111 Hospital Trusts surveyed, a mere 29% of coronary artery disease patients joined CR programmes.7 Our drop out rate from CR sessions of 26.49% is comparable to the study conducted by U.S Public Health Service,8 which also suggests that the understanding of the importance of CR is further enhanced when patients attended these sessions regularly.
The benefits of CR are multifactorial. The exercise regime helps to regress coronary atherosclerosis, improves coronary collateral circulation and endothelial dysfunction, and enhances the physiological and biochemical status of the cardiovascular system. The American Heart Association (AHA) recommends CR, a Class I indication for patients recovering after acute myocardial infarction or after coronary revascularization procedures. The AHA also emphasizes the need to identify patients who would most likely benefit from CR and also focus on their medical and social profiles to obtain maximum benefit and prevent drop-outs from the CR programmes.5
Our study showed that there was no significant gender difference in the attendance rates at CR, which was reported in previous studies.9 However, there was a significant association between the attendance rates and the cardiac clinical diagnosis/procedure as was noted in previous studies. It was observed that patients undergoing elective revascularization procedures (CABG or PCI) had a better attendance rate at CR (40.8%) as compared to the patients presenting with AMI and later undergoing CR (17.8%). Sundararajan et al10 noted that after CABG surgery, patients had a better attendance at the CR centers as compared to patients with other cardiac diagnosis,10 similar observations were noted in our study as the majority (57.4%) of the CR attendees had undergone CABG surgery. A possible reason could be that patients undergoing a surgical procedure considered their disease to be more serious as compared to those with other procedures and were more inclined to attend the sessions.
It was seen that the presence of a multitude of major coronary artery disease risk factors before the cardiac event, encouraged the patients to attend rehabilitation sessions. Attendance rate of diabetics (44.0%) and hypertensive patients (40.6%) in our study was much superior to those who did not have either of these risk factors. This possibly indicates that patients with co-morbid conditions considered themselves susceptible to future cardiac events and consequently attended these sessions more frequently. It may, however, be a bias from clinicians, who may consider these patients at higher risk and encourage cardiac rehabilitation. An interesting observation noted in a few other studies was that smokers tend to attend CR sessions less frequently than their non-smoker counterparts.11 This perhaps might be due to the fact that smokers are strongly instructed to quit smoking during the CR sessions. In comparison, the percentage of smokers was higher in our study compared to non-smokers; however this did not reach the level of significance.
Contrary to previous studies, attendance rates were not significantly affected by the financial status of the patient.12 It was previously noted that the unemployed (which included retired, housewives), were dependent on practical assistance for accessing the CR programme, which often lead to poor attendance13 however, this was not the case in our study, probably due to our culturally strong, closed-family support system and this is an encouraging factor that emerges from our study.
A vital factor which also has a considerable impact on CR attendance is easy access to the CR programme. Long distances from the CR centre would obviously deter consistent outpatient attendance as this would incur an additional cost of traveling to and from the CR center. This factor would be of significance to people participating in outpatient CR programmes of developing countries. Our study results are consistent with past reports which pointed out that patient with a comparably easy access to the CR centre had better attendance rates as compared to those having a more distant access to such centers.14
There are a few limitations to our study. Our study was a single centre study and a retrospective analysis of a small cohort of patients. Due to unavailability of local data, our findings could only be compared with that of foreign literature.
Conclusion
Results of our study highlight suboptimal outpatient cardiac rehabilitation attendance in a developing country cardiac center. Patients who underwent elective CABG surgery and who had easy access to the cardiac rehabilitation programme had better attendance rate. Factors contributing to poor attendance rates at CR programmes in developing countries need further exploration.
References
1. Jelinek M, Clark AM, Oldridge NB, Briffa TG, Thompson DR. Reconciling systematic reviews of exercise-based cardiac rehabilitation and secondary prevention programmemes for coronary heart disease. Eur J Cardiovasc Prev Rehabil 2011; 18: 147-9.
2. Balady GJ, Williams MA, Ades PA, Bittner V, Comoss P, Foody JM, etal.Core components of cardiac rehabilitation/secondary prevention programmes: 2007 update. A scientific statement from American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee, the Council on Clinical Cardiology, the Councils on Cardiovascular Nursing, Epidemiology and Prevention, and Nutrition, Physical Activity, and Metabolism, and the American Association of Cardiovascular and Pulmonary Rehabilitation. Circulation 2007; 115: 2675-82.
3. Linke A, Erbs S, Hambrecht R. Exercise and the coronary circulation-alterations and adaptations in coronary artery disease. Prog Cardiovasc Dis 2006; 48: 270-84.
4. Dendale P, Berger J, Hansen D, Vaes J, Benit E, Weymans M. Cardiac rehabilitation reduces the rate of major adverse cardiac events after percutaneous coronary intervention. Eur J Cardiovasc Nurs 2005; 4: 113-6.
5. Thomas RJ, King M, Lui K, Oldridge N, Piña IL, Spertus J, etal. AACVPR/ACC/AHA 2007 performance measures on cardiac rehabilitation for referral to and delivery of cardiac rehabilitation/secondary prevention services. J Am Coll Cardiol 2007; 50: 1400-33.
6. Cooper AF, Jackson G, Weinman J, Horne R. Factors associated with cardiac rehabilitation attendance: a systematic review of the literature. Clin Rehabil 2002; 16: 541-52.
7. Bethell H, Lewin R, Evans J, Turner S, Allender S, Petersen S. Outpatient cardiac rehabilitation attendance in England: variability by region and clinical characteristics. J Cardiopulm Rehabil Prev 2008; 28: 386-91.
8. Wenger NK, Froelicher ES, Smith LK, Ades PA, Berra K, Blumenthal JA, et al Cardiac rehabilitation as secondary prevention. Agency for Health Care Policy and Research and National Heart, Lung, and Blood Institute. Clin Pract Guidel Quick Ref Guide Clin 1995; 17: 1-23.
9. Thomas RJ, Miller NH, Lamendola C, Berra K, Hedbäck B, Durstine JL, et al. National Survey on Gender Differences in Cardiac Rehabilitation Programmes. Patient characteristics and enrollment patterns. J Cardiopulm Rehabil 1996; 16: 402-12.
10. Sundararajan V, Bunker SJ, Begg S, Marshall R, McBurney H. Attendance rates and outcomes of cardiac rehabilitation in Victoria, 1998. Med J Aust 2004; 180: 268-71.
11. Worcester MU, Murphy BM, Mee VK, Roberts SB, Goble AJ. Cardiac rehabilitation programmemes: predictors of non-attendance and drop-out. Eur J Cardiovasc Prev Rehabil 2004; 11: 328-35.
12. Higgins RO, Murphy BM, Goble AJ, Le Grande MR, Elliott PC, Worcester MU. Cardiac rehabilitation programme attendance after coronary artery bypass surgery: overcoming the barriers. Med J Aust 2008; 188: 712-4.
13. Hagan NA, Botti MA, Watts RJ. Financial, family, and social factors impacting on cardiac rehabilitation attendance. Heart Lung 2007; 36: 105-13.
14. De Angelis C, Bunker S, Schoo A. Exploring the barriers and enablers to attendance at rural cardiac rehabilitation programmes. Aust J Rural Health 2008; 16: 137-42.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: