
Muhammad Khalid Idrees ( Department of Nephrology, Sindh Institute of Urology and Transplantation, Karachi, Pakistan. )
Salma Batool ( Department of Molecular Biology & Immunology, Sindh Institute of Urology and Transplantation, Karachi, Pakistan. )
Ejaz Ahmed ( Department of Molecular Biology & Immunology, Sindh Institute of Urology and Transplantation, Karachi, Pakistan. )
December 2011, Volume 61, Issue 12
Original Article
Abstract
Objective: To study the characterstics, pattern of viral markers, hepatic transaminases and other associated hepatitis virus infections among maintainence haemodialysis patients.
Method: This prospective cross-sectional study was conducted at the dialysis unit of Sindh Institute of Urology and Transplantation Karachi on end-stage renal disease (ESRD) patients undergoing maintainence haemodialysis from November 2009 to April 2010. Patients on anti-viral drugs were excluded. Blood samples were taken, immediately before start of dialysis, for Hepatitis B virus serology, anti-HCV, polymerase chain reaction (PCR) for HBV DNA and biochemical tests. Abdominal ultrasound was performed for liver, spleen, portal vein diameter and presence or absence of ascites. Data analysis was done by using SPSS 10.0. The level of significance was taken as 0.05.
Results: Out of 1220 ESRD patients on maintainence haemodialysis at SIUT, 124 were HBsAg positive but 26 patients were excluded as they had received anti-viral therapy. Finally 98 patients including 71 (72%) males and 27 (28%) females completed the study. The mean age was 34.98±12.67 years. Most of the patients did not have hepatitis symptoms. ALT level was raised above cutoff value of 20 IU/ml in 62.2% patients while AST was raised in 75.4% patients. HBeAg was positive in 34.6%, anti-HBe antibody was positive in 65% patients and HBV DNA was detected in 65.3%. More than half of the patients had HCV co-infection. Six patients had cirrhosis. Thirty four patients were non-replicating carriers. The mean duration of dialysis and duration of HBsAg positivity were significantly longer in those patients who had hepatitis B and hepatitis C coinfection (p<0.05).
Conclusion: Hepatitis B virus infection in dialysis dependent patients is mostly asymptomatic. Mild transaminase elevation is frequently encountered.
Keywords: Hepatitis B, Haemodialysis, Serology, Polymerase chain reaction, Karachi (JPMA 61: 1210; 2011).
Introduction
Hepatitis B virus (HBV) infection is an exceptional threat for patients on haemodialysis and its presentation and clinical course in this group of patients is different from the general population.1 The patients on haemodialysis are at increased risk of acquiring HBV infection as compared to the general population.2 This is due to increased exposure to blood products, shared haemodialysis equipment, dialyser re-use, repeated needle insertions, breaching of skin and immunodeficiency. The prevalence and incidence of HBV infection among patients undergoing long-term haemodialysis is highly variable across different geographical regions, depending on local endemicity and enforcement of infection control measures in dialysis units. This ranges from 0.9% in US3 to 16.8% in Taiwan4 among dialysis patients. A countrywide survey5 conducted by Pakistan Medical Research Council estimated that 2.5% population is infected with hepatitis B virus. Pakistan is in the low HBV prevalence area. Little work has been done in Pakistan regarding HBV infection among dialysis dependent patients. A study from Islamabad6 revealed that 12.4% patients undergoing haemodialysis were hepatitis B surface antigen (HBsAg) positive and dialysis for more than 2 years was a significant risk factor.
Patients on maintainence haemodialysis and chronic HBsAg carriage rarely develop symptoms of hepatitis, are anicteric and have mild elevations of hepatic transaminase levels but silent hepatocellular injury continues.7 As the transaminase levels are usually depressed in patients undergoing maintainence haemodialysis, \\\'normal\\\' values of these enzymes may be indicative of a pathological state. Lopes and colleagues8 have recommended that the upper limit of normal (ULN) for alanine aminotransferase (ALT) be reduced. Patients with chronic hepatitis B infection are at an increased risk of developing liver cirrhosis, hepatic decompensation, and hepatocellular carcinoma9 Although many patients with end-stage renal disease (ESRD) do not live long enough to develop HBV-related complications, increased risk of hepatocellular carcinoma and mortality associated with HBV is reported in the ESRD population10 but it is controversial. There is only one study in literature which evaluated histopathological features in HBsAg positive haemodialysis patients.11 It has been shown that the level of HBV DNA is usually low among uraemic patients undergoing regular haemodialysis.12 Besides HBV infection, dialysis patients are prone to infection with other hepatotrophic viruses. A study from India13 showed that 3.7% dialysis dependent patients had HBV and hepatitis C virus (HCV) co-infection as compared to 1.4% HBV and 5.9% HCV patients.
This study was conducted to study the patients\\\' characteristics, pattern of viral markers and hepatic transaminases and associated other hepatitis virus infection among HBsAg positive dialysis patients at our institution.
Patients and Methods
This prospective cross-sectional study was carried out at the dialysis unit of Sindh Institute of Urology and Transplantation (SIUT) Karachi, Pakistan from November 2009 to April 2010. After approval from Ethical Review Committee of the institution, all the patients undergoing maintainence haemodialysis for at least 3 months were approached for inclusion in the study. Patients who had received anti-viral therapy were excluded. Patients with other causes of raised liver enzymes including alcohol, autoimmune hepatitis, haemochromatosis, primary biliary cirrhosis, primary sclerosing cholangitis, drugs (pyrazinamide, rifampicin, paracetamol), non alcoholic steato-hepatitis (NASH), Wilson\\\'s disease, alpha I antitrypsin deficiency, coeliac disease, recent surgery of hepatobiliary tract, and obstructed biliary tract were also excluded from the study. The whole procedure and purpose of the study and its potential implications were explained to the patients. The dialysis technicians and other staff members managing the HBsAg positive dialysis patients are restricted from managing HBsAg negative patients. These patients have twice or thrice weekly dialysis of 3.5-4 hours session with single use polysulfone dialyser of 1.2-1.6 micron. The dialysers and tubings are not re-used and not reprocessed. Patients were interviewed and their record checked for primary disease leading to ESRD, duration of dialysis, duration of known HBsAg positivity, blood transfusions before start of dialysis, prior surgery and history of jaundice. The patients were examined especially for jaundice, peripheral oedema and signs/stigmata of chronic liver disease. Blood samples were taken from the arterial line immediately after insertion of the needle (before dialysis was started) and plasma was separated in three aliquots, one for serological tests, one for PCR (polymerase chain reaction) and the third one for biochemical tests (ALT, AST, albumin, bilirubin, creatinine). Microparticle enzyme immunoassay (MEIA) Abbott ARCHITECT system was used for detection of HBsAg, IgM antibody to hepatitis B core antigen (anti-HBc IgM), anti-HBc total, hepatitis B e antigen (HBeAg), antibody to hepatitis B e antigen (anti-HBe antibody), antibody to hepatitis B surface antigen (anti-HBs antibody) and antibody to hepatitis C virus (anti-HCV antibody). A real time PCR artus HBV RG PCR kit from QIAGEN (detection limit=100 copies/ml) was used for the detection of HBV DNA. Serum asparate amintranseferase (AST), alanine aminotransferase (ALT), alkaline phosphtase, gamma glutamyltranspeptidase (GGT), total and direct bilirubin and other biochemical parameters were measured by standard laboratory techniques using an automatic analyzer.
Abdominal ultrasound was done in all the study participants and was reported by senior radiologist regarding size and echotexture of liver and spleen, portal vein diameter, presence or absence of ascites and splenic varices.
All the data was recorded in a pre-designed proforma and entered in SPSS 10 and analysed for frequencies of the variables. Student t-test was applied to compare the means of the study variables. The level of significance was taken as 0.05.
Results
At the time of present study, out of 1220 patients on maintainence haemodialysis at SIUT, 124 were HBsAg positive and were being dialysed on dedicated machines in hepatitis B positive dialysis unit. Twenty six patients were receiving or had received anti-viral therapy and were excluded from the study. Finally 98 patients (71 males, 27 females) were included in the study. Age of the patients ranged from 10 to 65 years (mean age: 34.98±12.67). The cause of ESRD in our study population was diabetes mellitus (21), renal stones (12), hypertension (11), glomerulonephritis (7), obstetric complications (4) and polycystic kidney disease (3). The cause of ESRD was not known in rest of the 40 cases who had bilateral small and shrunken kidneys at the time of first presentation.
These patients were on dialysis for 36.70±34.56 months. The mean duration of HBsAg positivity was 33.75±33.16 months. Seventy five patients were first time found to be HBsAg positive when they came for dialysis/renal replacement therapy at SIUT. Five patients had known HBsAg positivity before the start of dialysis. Eighteen patients, who were HBsAg negative at start of dialysis, had asymptomatic seroconversion to HBsAg positive state on routine interval screening. Fourteen out of these 18 patients had been intermittently dialysed at some other dialysis centers where hepatitis B positive patients were not segregated. None of the 98 patients were ever vaccinated against hepatitis B virus infection. Ten (10.2%) patients had history of blood transfusion before start of dialysis, while 20 (20.4%) patients had past history of surgery before start of dialysis. Eighteen (18.4%) patients had past history of jaundice.
Only 3 patients had clinically detectable jaundice at the time of the study. Liver was palpable in 9 patients and spleen in two patients. Stigmata of chronic liver disease (palmar erythema, gynaecomastia, loss of pubic hair) were present in two patients only. Result of liver function tests is shown in Table-1.
The median value of ALT was 27 U/l (IQR=16-46), with 26 patients having levels above 40 U/l. A similar pattern was seen in AST level where levels exceeding > 40 U/l was seen among 26 patients. Compared to transaminases (ALT and AST), GGT levels were higher with a median of 51.5 U/l (IQR= 27-88).
There were 56 hepatitis B patients who tested positive for hepatitis C antibody. Patients with hepatitis B and C co-infection had higher mean values for hepatic enzymes compared to isolated hepatitis B cases (Table-2),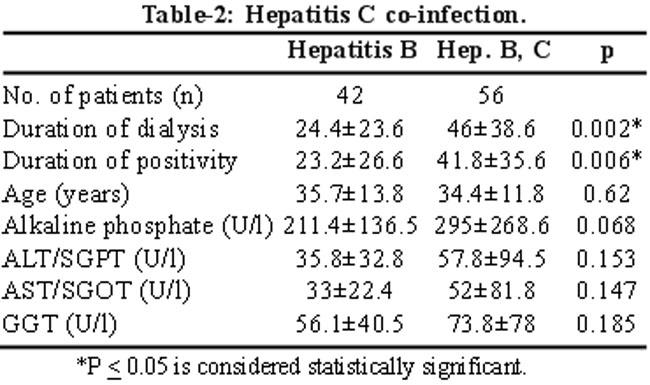
but failed to reach statistical significance. The only significant difference between the two groups was a relatively longer duration of dialysis dependency in patients with dual infection and by definition hepatitis B positivity.
Serologic markers in these patients are shown in Table-3.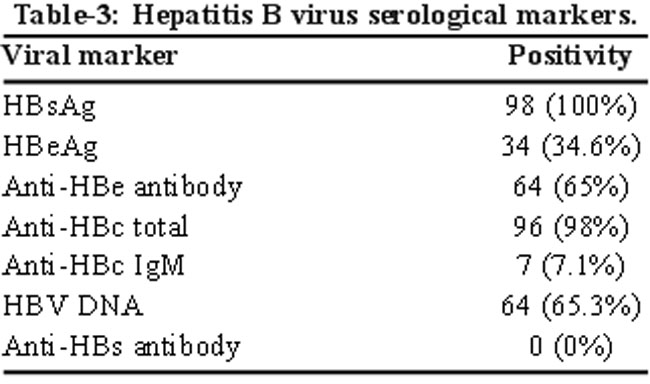
Anti-HBc IgM was present in 7 out of 96 subjects who tested positive for anti-HBc total. HBV DNA was positive in 64 patients with mean copy number of 2.3×109±9×109 copies/ml. Thirtyfour patients (34.6%) had both HBeAg and HBV DNA detectable, 30 patients had isolated HBV DNA positivity, while both were negative in 34 (34.7%) patients (Table-3).
On ultrasonography, 6 patients had features of liver cirrhosis while none of the patient had liver mass or hepatocellular carcinoma.
Discussion
To our knowledge, this is the first detailed study of hepatitis B positive dialysis dependent patients from our region. In this study, 10.2% (124 out of 1220) patients were HBsAg positive. This is in contrast to 2.5% HBsAg positivity in general population of Pakistan5 but closer to 12.4% HBsAg positivity among dialysis patients reported from a centre in Islamabad.6 Most of our patients had acquired hepatitis B virus infection before the start of dialysis. Majority of those who seroconverted to Hepatitis B positive state after commencing dialysis gave a history of dialysis at outside centres in between. Since only 3 of these patients had anti-HBc IgM, the remainder must have acquired infection much earlier than in the present study. An alternative explanation is latent infection at the time of commencing dialysis when they may have had low titre HbsAg undetected by usual testing and were mislabelled as HBsAg negative. This high frequency of HBsAg positivity among our dialysis patients is probably because of lack of clearance of HBV infection due to uraemic state.1 Selective referral of HBsAg positive ESRD patients from dialysis centres who do not dialyse positive patients is another major reason of high prevalence in our study. Not all the dialysis units in Pakistan have the facility for dialysing HBsAg positive patients. According to dialysis registry of Pakistan 2010, only 34.46% (51 out of 148) dialysis units in Pakistan provide dialysis facilities to HBsAg positive patients.14 In this situation, HBsAg positive ESRD patients are referred to SIUT as it has a dedicated HBsAg positive dialysis unit.
The majority of patients in our study were males. Men have greater opportunities for seeking medical help and in addition, there is gender difference in the prevalence of hepatitis B infection in general population with males outnumbering the females.15
Duration of dialysis dependency was significantly longer for patients with hepatitis B and C co-infection than patients with hepatitis B infection alone. A study from Taiwan4 found that dialysis patients with dual infection (hepatitis B and C) are younger, have longer duration of dialysis and more severe liver dysfunction as compared to those with HBV infection alone. We also found higher levels of hepatic transaminases in patients with dual infection as compared to those with hepatitis B infection alone but it failed to reach the level of statistical significance.
Most of the patients did not have symptoms of liver disease or hepatitis and only 3 patients had clinically detectable jaundice and raised serum bilirubin level. It is well described in the literature that dialysis patients may progress to chronic hepatitis or chronic liver disease without having any clinical features.7 Although transaminase levels were checked once in the study period, there was wide variation in its levels, and it ranged from below normal to many folds raised. We had excluded other causes of raised liver enzymes including alcohol, autoimmune hepatitis, haemochromatosis, primary biliary cirrhosis, primary sclerosing cholangitis, drugs (pyrazinamide, rifampicin, paracetamol), non alcoholic steato-hepatitis (NASH), Wilson\\\'s disease, alpha I antitrypsin deficiency, coeliac disease, recent surgery of hepatobiliary tract, and obstructed biliary tract. In our study population 62.2% patients had ALT level above the cutoff value (20 U/l) for dialysis patients and 75.4% had AST level above the cutoff value of 20 U/l for dialysis patients. Usually the levels of hepatic enzymes have been described to be low among HBV infected dialysis patients because of the removal of these enzymes by process of dialysis but certain studies have found raised levels of hepatic transaminases among this patient population.16 However it has also been observed that ALT level rises after dialysis because of haemo-concentration as the fluid is removed in ultrafiltration. Lopes et al8 suggested that the upper limit of the normal ALT level for dialysis patients should be reduced by 40% relative to the upper limit of normal for general population if the blood samples are collected before the haemodialysis session or by 60% if blood samples are collected after the dialysis session.
In our study, HBeAg was positive in 34 (34.6%) HBsAg positive patients and anti-HBe antibody was positive in 64 (65%) patients while HBV DNA was detected in 64 (65.3%) patients. Thirty four (34.7%) patients were non-replicating carriers of hepatitis B virus as both HBeAg and HBV DNA were un-detectable in these patients. HBsAg positive patients with negative HBeAg and undetectable HBV DNA are labeled as non-replicative hepatitis B virus (inactive) carriers. The lower limit of detection of DNA copy numbers by PCR used in our laboratory was 100/ml, and it is possible that they may well be replicating at a very slow rate resulting in less than 100 copies/ml. There is paucity of data about replicative status of hepatitis B positive dialysis patients. Our results closely resembles a study from central Brazil17 that found that 34.6% of HBsAg positive dialysis patients were HBeAg positive, 57.7% were anti-HBe positive and 65.4% had HBV DNA detectable by PCR. Large scale studies are needed to find the exact pattern of HBV markers and proportions of various stages of HBV infection among HBsAg positive dialysis patients.
Most of the HBsAg positive patients (86.7%) in our study were asymptomatic carriers of hepatitis B (non-replicating and replicating). Six of our patients had liver cirrhosis. These patients were dialysis dependent and HBsAg positive for 8 to 10 years. Degott and colleagues in a histological study11 of HBsAg positive dialysis patients found that 72% patients developed biopsy proven chronic hepatitis over a period of 8 years follow up. A study from China18 found that although dialysis dependent patients did not eliminate the hepatitis B virus, the prognosis for patients with HBV is good and cirrhosis or hepatoma did not occur among the patients in that study after follow up of 39.45 ± 7.57 months.
A study from Egypt19 also had similar findings and none of the HBsAg positive dialysis patients (on dialysis for a mean duration of 36.53±9.45 months) developed cirrhosis, hepatocellular carcinoma (hepatoma) or decompensation of liver function. The finding of cirrhosis in our patients may be due to prolonged duration of HBV infection and concomitant HCV infection in 3 out of 6 cases. Hepatitis C co-infection is known to accelerate the progression and severity of liver disease among dialysis dependent patients.4,20
Conclusion
Hepatitis B virus infection in dialysis dependent patients is mostly asymptomatic. Though mild transaminase elevation is frequent, long term follow up is necessary to assess the risk for development of chronic liver disease. With the availability of new drugs, selective treatment of at risk group can be initiated.
References
1.Wong P, Mak S, Wong AK. Management of chronic hepatitis B infection in patients with end-stage renal disease and dialysis. Hep B Annual. (Online) 2006 (Cited 2011 Jan 5). 3: 76-105.
2.Edey M, Barraclough K, Johnson DW. Hepatitis B and dialysis. Nephrology (Carlton) 2010; 15: 137-45.
3.Tokars JI, Finelli L, alter MJ, Arduino MJ. National surveillance of dialysis-associated diseases in the United States, 2001. Semin Dial 2004; 17: 310-9.
4.Chen KS, Lo SK, Lee N, Leu ML, Huang CC, Fang KM. Superinfection with hepatitis C virus in hemodialysis patients with hepatitis B surface antigenemia: Its prevalence and clinical significance in Taiwan. Nephron 1996; 73: 158-64.
5.Qureshi H, Bile KM, Jooma R, Alam SE, Afridi HUR. Prevalence of hepatitis B and C viral infections in Pakistan: findings of a national survey appealing for effective prevention and control measures. Eastern Mediterranean health J 2010; 16: S15-23.
6.Khokhar N, Alam AY, Naz F. Hepatitis B surface antigenemia in patients on hemodialysis. Rawal Med J 2004; 29: 18-21.
7.Fabrizi F, Lunghi G, Martin P. Hepatitis B virus infection in hemodialysis: recent discoveries. J Nephrol 2002; 15: 463-8.
8.Lopes EP, Sette LH, Sette JB, Luna CF, Andrade AM, Moraes M, et al. Serum alanine aminotransferase levels, hematocrit rate and body weight correlations before and after hemodialysis session. Clinics (Sao Paulo) 2009; 64: 941-5.
9.Yu MW, Hsu FC, Sheen IS, Chu CM, Lin DY, Chen CJ, et al. Prospective study of hepatocellular carcinoma and liver cirrhosis in asymptomatic chronic hepatitis B virus carriers. Am J Epidemiol 1997; 145: 1039-47.
10.Jha R, Kher BA, Naik S, Elhence R, Gupta A, Sharma RK. Hepatitis B associated liver disease in dialysis patients: Role of vaccination. J Nephrol 1993; 6: 98-103.
11.Degott C, Degos F, Jungers P, Naret C, Courouce AM, Potet F, et al. Relationship between liver histopathological changes and HBsAg in 111 patients treated by long-term hemodialysis. Liver 1983; 3: 377-84.
12.Tseng GY, Lin HJ, Fang CT, Cheng YT, Huang CH, Tseng GC, et al. Hemodialysis reduces the viral load in uremic patients with chronic hepatitis B infection. Ren Fail 2008; 30: 1000-5.
13.Reddy GA, Dakshinamurthy KV, Neelaprasad P, Gangadhar T, Lakshmi V. Prevalence of HBV and HCV dual infection in patients on haemodialysis. Indian J Med Microbiol 2005; 23: 41-3.
14.Dialysis registry of Pakistan 2010. The kidney foundation. Karachi. (Online) 2010 (Cited 2011 Jan 5). Available from URL: http://www.kidneyfoundation.net.pk/dialysis_2010.pdf.
15.Baig S. Gender disparity in infections of hepatitis B virus. J Coll Physc Surg Pak 2009; 19: 598-600.
16.Bosevska G, Kuzmanovska G, Sikole A, Dzekova-Vidimilski P, Polenakovic M. Screening for hepatitis B, C and HIV infection among patients on haemodialysis (cross sectional analysis among patients from two dialysis units in the period January to July 2005). Prilozi 2009; 30: 159-74.
17.Ferreira RC, Teles SA, Dias MA, Tavares VR, Silva SA, Gomes SA, et al. Hepatitis B virus infection profile in hemodialysis patients in Central Brazil: prevalence, risk factors, and genotypes. Mem Inst Oswaldo Cruz 2006; 101: 689-92.
18.Cao YL, Wang SX, Zhu ZM. Hepatitis B viral infection in maintenance hemodialysis patients: a three year follow-up. World J Gastroenterol 2007; 13: 6037-40.
19.Elghannam DM, Aly RM, Goda EF, Eltoraby EE, Farag RE. Clinical significance of antibody to hepatitis B core antigen in multitransfused hemodialysis patients. Asian J Transfus Sci 2009; 3: 14-7.
20.Bini EJ, Perumalswami PV. Hepatitis B virus infection among American patients with chronic hepatitis C virus infection: Prevalence, racial/ethnic differences, and viral interactions. Hepatology 2010; 51: 759-66.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: