
Amber Mehmood ( Department of Emergency Medicine, Aga Khan University Hospital, Karachi. )
Syed Muhammad Baqir ( Department of Emergency Medicine, Aga Khan University Hospital, Karachi. )
Muhammad Shahid ( Department of Emergency Medicine, Aga Khan University Hospital, Karachi. )
Junaid Abdul Razzak ( Department of Emergency Medicine, Aga Khan University Hospital, Karachi. )
November 2011, Volume 61, Issue 11
Special Communication
Abstract
Although Emergency Medicine (EM) is an integral part of undergraduate medical curriculum in many countries, it has not been included formally in the MBBS curriculum in Pakistan. Medical graduates are supposed to be able to handle common as well as life threatening emergencies but little has been done to ensure the process to achieve this competence. The development of an undergraduate EM curriculum is important but challenging task. Implementation of standard curriculum will ensure that medical graduates have gained competence in assessing and managing acutely ill patients and dealing with common emergencies. This paper shares the features of an undergraduate EM clerkship which can be used as a template by other medical institutions.
Keywords: Emergency medicine, Medical curriculum, Medical graduates, Pakistan.
Introduction
In 1994, Macy Foundation Conference was held to define the future of Emergency Medicine (EM). One of the recommendations was to "…. ensure that every medical student has acquire the appropriate knowledge and skills to care for emergency patients."1 EM has evolved over time into a highly sought, competitive discipline and has become the source of diverse learning opportunities for medical students; from prehospital care to resuscitation, medical toxicology, disaster medicine and paediatric EM, just to name a few.2 EM has not been the focus of local medical curriculum and to date no Pakistani medical college in public sector has a formal undergraduate EM Clerkship programme.3 So far, the Department of Emergency Medicine at the Aga Khan University, Karachi is the only academic department to have integrated EM into the undergraduate medical education.
In this paper, we report the goals and objectives, teaching methods and evaluation process of our programme, and briefly discuss the lessons learnt through this experience.
Goals and Objectives:
The main goal of clerkship is to enable the medical students to recognize life threatening medical emergencies, prioritize patient care and apply principles of resuscitation in critically ill and injured patients. The objectives are achieved by exposing the students to the diagnostic and management approach to an acutely ill and undifferentiated patient through focused history and physical examination, relevant investigation and interpretation, planning and execution of a management plan and understanding the disease process from a patho-physiological stand point rather than arriving at discrete diagnoses.
Methods
Course Organization:
Every three months there is a batch of students who rotate through EM for four weeks. The students are divided into smaller groups to be distributed in different shifts and exposed to patients with different acuity of disease. An end-of shift case discussion with the on-call faculty member usually supplements the learning needs of each student. Students are instructed to keep a log of their cases, procedural skills and patient encounters.
Course Content:
The course includes formal didactic sessions which are based on clinical presentations rather than specific diseases, bedside teaching, a two days Advance Cardiac Life Support workshop, assessment of trauma patients and spinal immobilization (Table).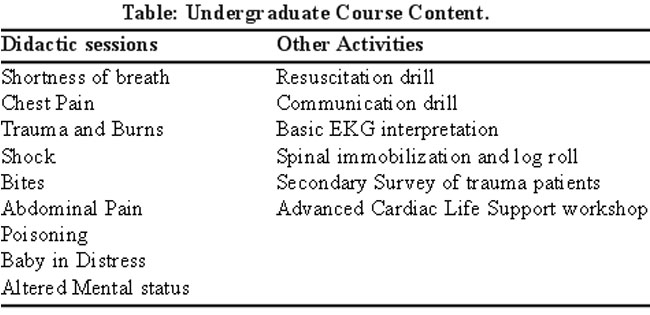
The students learn indications and complications of basic procedural skills such as blood sampling, NG tube placement, arterial sampling, venous access and Foley\\\'s catheterization, and perform these procedures under supervision.
Evaluation Methods:
Generally students\\\' evaluation is based on attendance, an OSCE based end-of term exam, and case presentations. Shift evaluation, logs and direct observation lead to a formal mid-term feedback for individual students.
Results
Until 2010, four batches of final year medical students have gone through this rotation and have participated in the formal evaluation process. This means that so far, more than 400 medical graduates have received basic EM as well as advanced life support training. Clearing the ACLS is the pre-requisite to appear in the end of term exam. Failure to pass the rotation requires a remedial period of clerkship and reappearance in the/a repeat [recommended by AFQ] OSCE exam.
Discussion
Until recently Emergency Medicine as a specialty was awaiting recognition in Pakistan. This affects not only undergraduate training but also the quality of care provided in emergency rooms.3 Although there is currently no recognized standard curriculum for the undergraduate emergency training,4 we faced a dual challenge of choosing the most essential content and ensuring that this is also fulfils local needs. We designed this clerkship based on the available guidelines to provide the core knowledge and skills.5,6 Before implementation, formal approval from the University MBBS curriculum committee was sought. The designing, implementing and administering of this clerkship required dedicated faculty time, formal training in the field of education and administrative support by the University.
Keeping the curriculum short yet comprehensive and deliver the knowledge in all required fields with a formal evaluation process were the greatest challenges. Assignment of medical students in different patient care areas of varying acuity ensures that they are able to see a wide case mix.7 To help students deal with stressful situations, they were encouraged to participate actively in resuscitation and to observe communications with family in an environment which is unique to the emergency room. Continuous modifications were made in the clerkship programme, based on formal feedback of the rotation by the students. An increasing number of students applying for the EM electives is an indirect corroboration of the popularity of this clerkship.
The expectation that all medical graduates are capable of handling medical emergencies remains unfulfilled when the required training is not incorporated into the curriculum. Most of the medical students report improvement in providing basic life support, diagnosis and treatment of acute undifferentiated illnesses, and provision of basic trauma care after an undergraduate EM rotation.8,9 Incorporation of an EM training module in undergraduate medical curriculum provides students with basic science and clinical knowledge, improves psychomotor skills, and help defining their future interests in EM as a specialty.10 Once well established, the scope can be expanded to include EM modules in years III and IV curricula as well as electives in EM specialties such as pre-hospital care, trauma, paediatric EM, toxicology, research and injury prevention.2,8
Conclusion
Capacity building in medical education has been shown to improve the delivery of health care as well as improvement in quality of care. This calls for action for national medical curriculum development committees to develop an undergraduate EM curriculum which is according to international guidelines as well as contextual to local needs.
References
1.Macy JJr. The role of emergency medicine in the future of American medical care. Ann Emerg Med 1995; 25: 230-3.
2.Pacella CB. Advanced Opportunities for Student Education in Emergency Medicine. Acad Emerg Med 2004; 11: 1028.
3.Razzak JA, Ahmed A, Saleem AF, Nasrullah M. Perceived need for emergency medicine training in Pakistan: A survey of medical education leadership. Emerg Med Austral 2009; 21: 143-6.
4.Hobgood C, Anantharaman V, Bandiera G, Cameron P, Halperin P, Holliman J, et al. International Federation for Emergency Medicine model curriculum for medical student education in emergency medicine. Emerg Med Austral 2009; 21: 367-72.
5.Manthey DE, Coates WC, Ander DS, Ankel FK, Blumstein H, Christopher TA, et al. Report of the Task Force on National Fourth Year Medical Student Emergency Medicine Curriculum Guide. Ann Emerg Med 2006; 47: e1.
6.Burdick WP, Jouriles NJ, D\\\'Onofrio G, Kass LE, Mahoney JF, Restifo KM. Emergency medicine in undergraduate education. Acad Emerg Med 1998; 5: 1105-10.
7.Coates WC. An educator\\\'s guide to teaching emergency medicine to medical students. Acad Emerg Med 2004; 11: 300-6.
8.Celenza A, Jelinek GA, Jacobs I, Kruk C, Graydon R, Murray L. Implementation and evaluation of an undergraduate emergency medicine curriculum. Emerg Med (Fremantle) 2001; 13: 98-103.
9.Lin HL, Chen CW, Lee WC, Kuo LC, Cheng YC, Lin YK, et al. Effects of the Emergency Trauma Training Course on the Confidence of Final-Year Medical Students Dealing with Trauma Patients. Kaohsiung J Med Sci 2009; 25: 10-5.
10.Gallagher EJ, Goldfrank LR, Anderson GV. Role of emergency medicine residency programs in determining emergency medicine career choice among medical students. Ann Emerg Med 1994; 23: 1062-7.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: