
Anwar T. Merchant ( Department of Community Health Sciences, The Aga Khan University, Karachi. )
lrfan Lalani ( Department of Medical Students, Class of 1999, Medical College, The Aga Khan University, Karachi. )
Zahid H. Afridi ( Department of Medical Students, Class of 1999, Medical College, The Aga Khan University, Karachi. )
Nida Latif ( Department of Medical Students, Class of 1999, Medical College, The Aga Khan University, Karachi. )
Talha A. Malik ( Department of Medical Students, Class of 1999, Medical College, The Aga Khan University, Karachi. )
Shehazad S. Merchant ( Department of Medical Students, Class of 1999, Medical College, The Aga Khan University, Karachi. )
lnayat A. Momin ( Department of Medical Students, Class of 1999, Medical College, The Aga Khan University, Karachi. )
Sonia S. Moizuddin ( Department of Medical Students, Class of 1999, Medical College, The Aga Khan University, Karachi. )
Arashk Motiei ( Department of Medical Students, Class of 1999, Medical College, The Aga Khan University, Karachi. )
Shaheen Motiwala ( Department of Medical Students, Class of 1999, Medical College, The Aga Khan University, Karachi. )
Asma Munir ( Department of Medical Students, Class of 1999, Medical College, The Aga Khan University, Karachi. )
Ayesha K. Sethi ( Department of Medical Students, Class of 1999, Medical College, The Aga Khan University, Karachi. )
April 2000, Volume 50, Issue 4
Original Article
Abstract
Objective: Occupational hearing loss is common in the industrialized world. Road noise is a major contributor to perceived environmental noise. The objective of this study was to assess hearing loss in rickshaw drivers due to rickshaw noise.
Methods: Hearing loss in rickshaw drivers and taxi drivers of Karachi who were 50 yeats of age or younger was estimated, with a Smith Hearing Screening (SHS) questionnaire that was modified, translated into the national language, Urdu and field tested prior to administration.
Results: Interviews for 91 rickshaw drivers and 94 taxi drivers were completed. All subjects were male; mean ages were 34 and 33 years for rickshaw and taxi drivers respectively. None of the rickshaws were fitted with silencers. Rickshaw drivers were about thrice as likely to he screened as hearing impaired by the SHs questionnaire (RR 2.9, 95% confidence interval 1.6, 5.0), twice as likely to report tinnitus (RR 2.2, 95% confidence interval, 1.1, 3.3) and two and a half times as likely to have difficulty in following telephonic conversations (RR 2.4, 95% confidence interval 1.2, 4.8).
Conclusion: There is loss of hearing and tinnitus among rickshaw drivers that could be attributed to their trade. Use of silencers by rickshaw drivers could result in less hearing loss among rickshaw drivers and less noise in the environment for the other 11 million residents in the city UPMA 50:1 24, 2000).
Introduction
Exposure to high levels of noise is associated with tinnitus and permanent hearing loss1 as well as sleep disturbances2, hypertension3,4. psychological disturbances5 and increased accidents on the job6. Noise damages, initially, the outer hair cells of the cochlea. If exposure persists for sufficient periods, the inner ear structures including all types of cells in the organ of corti and most cell types in other intracochlear structures such as the stria vascularis, spiral ligament and spiral prominence are also damaged7.
Occupational hearing loss is common in the industrialized world, it is eight among leading occupational diseases or injuries in the United States8. In the UK there were an estimated 1.7 million individuals with impaired hearing in 19929. Both these countries have hearing conservation laws, noise reduction programs at worksites and measures to reduce noise in the environment10. Similar effective programs are absent in Pakistan.
Road noise is a major contributor to perceived environmental noise. Traffic contributes to noise in the environment resulting in psychological and sleep disturbances5. In England and Wales in 1986 the department of Environment quoted 11420 offenses related to noise from motor vehicles, 90% of which involved faulty silencers9. A rickshaw is a light-weight, three wheeled taxi, with a two stroke engine, for two passengers, which costs less to use than the conventional four-wheeled taxi; it is commonly used in all major cities of Pakistan, except Islarnabad, where it is banned. In Karachi, rickshaw drivers remove rickshaw silencers to gain extra mileage; it has a noise level of 90dB inside the vehicle. Karachi. Pakistan’s largest city. is located in the province of Sindh, where 49% of the countries 68,183 rickshaws are registered11. By contrast Sindh has 3 1% of the country’s conventional four-wheeled taxis11. The result is a noisy environment. Rickshaws, apart from increasing the noise level of the environement, are also likely to effect the passengers, passersby and its drivers; the latter probably constitute a particularly high risk group for noise induced morbidity.
One constraint in assessing the effects of noise as a public health problem in Pakistan is that they are difficult to measure. Noise induced hearing loss is best assessed by audiometry12 which is not very accessible to many people in Pakistan. Alternative instruments, like questionnaires, have been used for screening of hair loss13-15 in other settings. One such questionnaire, developed by Smith and co-workers was used in this study15, to compare the prevalence of hearing impairment in rickshaw and taxi drivers in Karachi. The objective of this study was to assess hearing loss in rickshaw drivers due to rickshaw noise.
Methods
We enrolled rickshaw and taxi drivers of’ Karachi who were 50 years of age or younger. Workers over 50 years of age were excluded from the study. in order to minimize the contribution of presbycusis to measured hearing loss. Rickshaw drivers were considered exposed if they have driven a rickshaw for two more years (exposed group). They were compared to taxi drivers who had never driven a rickshaw for a living (unexposed group). All the subjects were interviewed in November 1995 at four sites in Karachi where rickshaws and taxis wait for their clients.
Hearing loss was assessed with a Smith Hearing Screening. (SHS) questionnaire15 that was modified. translated into the national language. Urdu and field tested prior to administration. The SHS questionnaire has been tested against a pure tone screening device, the Welch Allyn Audioscope, with a reported sensitivity ol 70.8% and specificity of 92.8%15. A copy of the questionnaire we used is attached as appendix1.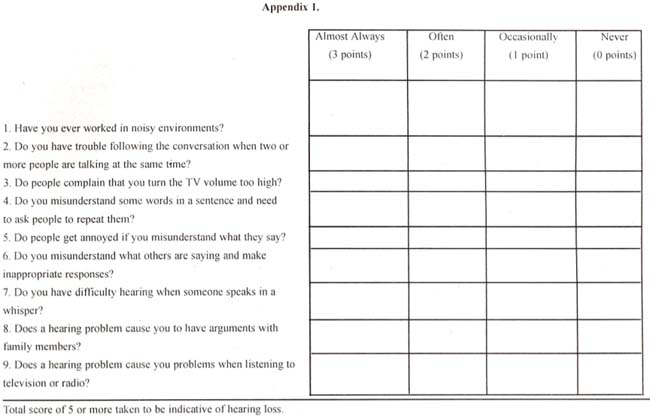
After field testing we retained 9 of the 14 questions of the SHS questionnaire. We dropped items in the SHS questionnaire that related to social activities and visitiiig friends as we found in the pre-test that rickshaw and taxi drivers had little time for social interaction or to meet new people. As on the SHS questionnaire, each question was scared on a scale of 0 to 3, making 27 the maximum score a person could obtain on our modified questionnaire as compared to 42 on the original SHS questionnaire. Persons scoring 6 or more on the SHS questionnaire are classified as hearing impaired. Since we reduced the number of questions, we took a score of 5 or more to indicate hearing impairment.
By comparing proportions of prevalence in the exposed and unexposed groups we estimated that we needed 142 subjects. 71 rickshaw and 71 taxi drivers, to measure a relative risk of 3, assuming the prevalence of hearing loss to be 1 0% in the unexposed group (taxi drivers), with an alpha error of 0.05 and a power of 0.8. As we had no previous studies6 to guide us, we based our assumptions on the data obtained in pre-testing. We interviewed 96 rickshaw and 99 taxi drivers. The data were edited in the field and entered and analyzed in Epi Info Version 616.
We used relative risks to compare the differences between rickshaw and taxi drivers with respect to those who scored 5 or more on the modified SHS questionnaire (hearing impaired) and those scoring less than 5 (not hearing impaired) and other outcomes associated with noise exposure like frequent headaches. tinnitus and reported difficulty in following telephone conversations. We stratified our results on the basis of those who were in their respective professions for six or fewer years and more than six years and calculated a summary relative risk for the combined strata with the Mantel-Hanszael method.
Results
Out of those who completed the interviews 5 rickshaw and 5 taxi drivers who were more than 50 years old; were excluded from the analysis. ihis left us with 91 exposed (rickshaw drivers) and 94 unexposed (taxi drivers) subjects on whom we did the analysis. All the subjects were male. The youngest rickshaw and taxi drivers were 1 8 and 20 years old respectively; 75% were more than 26 and 27 years of age respectively. None of the rickshaws were fitted with silencers. I3oth rickshaw and taxi drivers worked on average for about 11 hours a day, six and a half days a week. Rickshaw drivers, however had been in the trade for an average of about twelve years as compared to about six yeas for taxi drivers (Table 1).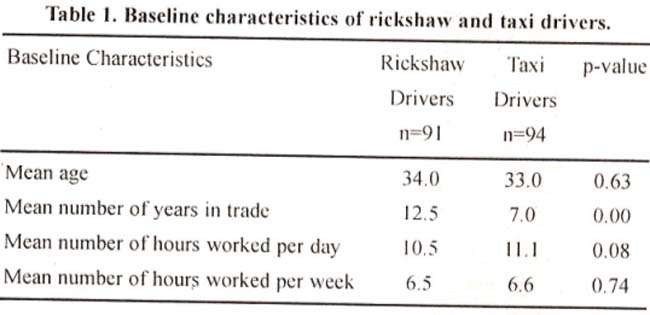
Rickshaw drivers scored higher on average than taxi drivers on the modified SHS instrument (5.4 versus 2.9, p-value 0.00). Rickshaw drivers were about thrice as likely as taxi drivers to be screened as hearing impaired using the modified SHS questionnaire, about twice as likely to report ringing of the ears and about two and a half times as likely to have difficulty in following a telephonic conversation (table 2).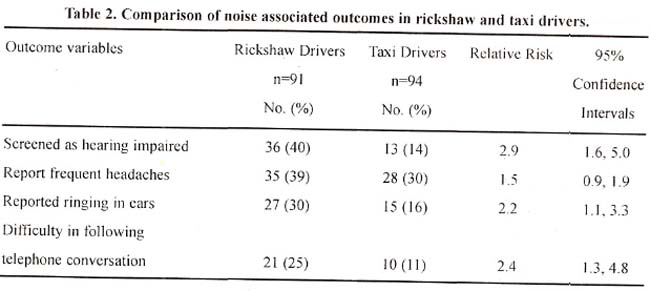
Among those in the trade for six years or less, rickshaw drivers were more than two and a half times as likely to be screened as hearing impaired as compared to taxi drivers (RR 2.6, 95% confidence interval 1.3. 5.3). Among those in the trade for more than six years, rickshaw drivers were more than four times as likely to be hearing impaired as compared to taxi drivers (RR 4.4, 95% confidence interval 1.4, 13.6). We combined the groups of those in the business for six years or more and calculated a Mantel-Hanszael summary relative risk; we found that on the whole rickshaw drivers were more than three times as likely to be hearing impaired as compared to taxi drivers (Mantel-Hanszael summary relative risk 3.3, 95% confidence interval 1 .8, 6.3).
Discussion
We assessed the effect of occupational noise on rickshaw and taxi drivers using three parameters; the SHS questionnaire, reported tinnitus and reported difficulty in following telephonic conversations. We consistently found that rickshaw drivers were more likely to be hearing impaired.
The SHS questionnaire has a sensitivity of 80.8% and a specificity of 92.6% against a Welch Allyn Audioscope. We modified the SHS questionnaire, reducing the number of questions from 14 to 9. We still found a strong association between rickshaw driving and hearing impairment. This finding would not result from an imprecise instrument to detect hearing loss. Indeed, an imprecise instrument would randomly misclassify both rickshaw drivers and taxi drivers and lead to an underestimate of the true association between rickshaw driving and hearing loss.
In this study we did not eliminate persons with existing hearing impairment that was not associated with noise, for example wax in the ears and nerve damage. There is no reason for us to believe, however, that the prevalence of these conditions would differ in the two groups. This being the case, not eliminating such cases would again lead to an underestimate of the true effect of the exposure on the outcome.
Because some of the subjects in our sample could not read, this questionnaire was administered by interviewers. Since they knew the hypothesis that was being tested, they could be a potential source of bias. To reduce potential interviewer bias we used structured questions and practiced administering the questionnaire. Moreover, the classification as hearing impaired, made by assigning a score for each individual was done after the interview.
We chose taxi drivers as a comparison group because they were exposed to the same level of background traffic noise as the rickshaw drivers. The only difference between these groups was that rickshaw drivers had, on average, been in trade for a longer time than taxi drivers. We stratified into groups of rickshaw and taxi drivers in the trade for less than six years and those in the business for six years or more and found that exposure to the high noise level of a rickshaw (about 90 dB) remained independently predictive of hearing loss.
The financial profit to the rickshaw drivers, by removing silencers and gaining extra mileage, is offset by a loss in their hearing. This point needs to be publicized among them and among the general public. With public pressure rickshaw drivers may be persuaded to use silencers which would result in less hearing loss for them and less noise in the environment for the other 11 million residents of the city.
Acknowledgements
We are grateful to Drs. Stephen Luby and Arnanullah Khan for reviewing the manuscript and offering valuable suggestions.
References
1.Clark WW Heanng: the effects of noise. OtoIaryngol cad Neck Surg 1992; 106:669-676.
2.Alster J, Shcmesh Z. Oman M. et al Sleep disturbance associated wills chronic tinnitus. Biol. Psychiatry, 1993:34:84—90.
3.Altura 13M, Altura BT, Gebrewold A, et at. Noise—induced hypertension and magnesium in rats: relationship to microcirculatioti and calcium J. AppI. Physiol.. 992:72: 94-202.
4.Wit CC. Chen SJ, Yen MH. Effects of’ noise ott blood pressure and ascular reactivities, Clin. Exp. Pharmacol. Thysiol.. 1 992:1 9:83-38
5.Slansfeid SA, Sharp OS, Gallacher J, et ali. Road traffic noise, noise sensitivity and psychological disorders. Psychol. N-led., 1993:23:977-85.
6.Melamed S. Luz J, Greets MS. Noise exposure. noise anttovattce and their relation to psychological distress, accident and sickness absence among blue— collar workers - the Cordis study. tsr. J. Med. Sci., 992,28:629-35
7.Brookhauscr PE, Worthittgton OW, Kelly WJ . Noise-induced searing loss in children. Laryngoscope, 1992:102:645-55.
8.Monson RR. Occupational Epidemiology, Boca Raton, Florida, CRC Press Inc., 1990,p.214.
9.Godlee F. Noise, breaking the silence Br. Med. J,, 1992:304: 110-13.
10.Hansen JA. OSHA regulation of ergonomic health J. Occup. Med.,
1993:3542-46.
.11.Pakistan Stasticial yearbook 995• Islamabad. Federal Bureau of Statistics, E.onomic Affairs and Statistics division, 1996. p. 216.
12.Adera T, Donahue AM, Malit B D. et at. Assessment of the proposed l)raft American National Standard method of evaluating the effectiveness of hearing conservation programs. i. Occup. Med., 1993.35:568-73.
13, Mc Bride WS, Mulrow CD. Aguilar C, et at. Methods for screening for hearing toss in older adults. Am. 3. Med. Sci . 1994:307:40-42.
14.Smeltzer CD, Pnmarv care screening and evaluation of hearing loss. Nurse Praci., 1993:18:50-55.
15.Smith MF, Nathan R(i, Wayner DS, et at. Comparative validity of two hearing loss screening questionnaires J. Fam Pract . 992:35.41 1-16.
16.Epi Info Version 6,02. Centres for D isease Control, Atlanta, Georgia. 1994.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: