
Ambreen Moatasim ( Department of Histopathology, PNS Shifa Hospital, Karachi. )
July 2011, Volume 61, Issue 7
Case Series
Abstract
Renal cell carcinomas (RCC) have been considered as a single entity, until recently. Today, however, these are not considered as a single tumour but instead represent various distinguishable entities, each having unique histology, cytogenetic and molecular features. The variants of renal cell carcinoma can be easily recognized histologically and hence one can identify tumours having similar clinical course, morphology, genetics, prognosis and possibly treatment. This descriptive study carried over a period of one and a half year at Shifa International Hospital, Islamabad, focuses on presenting our data of various variants of renal cell carcinoma and the need for their recognition as the correct diagnosis may help to modify the therapeutic protocol. During the study period a total of 13 cases of RCC were diagnosed with the clear cell variant as the most frequent type (n = 9; 69.2%). There was one case each of chromophobe renal carcinoma, medullary carcinoma, mucinous tubular and spindle cell carcinoma and multilocular cystic renal carcinoma. The average size of tumour ranged from 2.8 cm to 9.0 cm. Furhman\\\'s nuclear grade 2 was most frequently encountered (n= 6; 46 %) while the most frequent pathologic tumour stage was pT2 (n=7; 54%). This series is limited due to small sample size. More such studies on a larger scale with incorporation of follow up data are recommended to obtain population based statistics and identify biologically favourable variants in which nephron sparing surgery may be a suitable option.
Keywords: Renal cell carcinoma, Chromophobe renal carcinoma, Medullary carcinoma, Mucinous tubular carcinoma, Spindle cell carcinoma.
Introduction
Amongst renal tumours, renal cell carcinoma constitutes the most frequent diagnosis that is about 90 % and occurring in adults in both sexes. Although no authentic data for the prevalence of renal cell carcinoma in Pakistan is available, one study carried out at Aga Khan University Hospital, Karachi on 2393 cases of solid malignancies showed a frequency of 1.8% amongst males.1 The purpose of classifying renal tumours is to identify tumours having similar course, prognosis and possibly treatment. Current advances in molecular studies and cytogenetics justifies grouping of prognostically similar tumours arising from unique cell types. Today these tumours are considered as various distinguishable entities,2,3 each having unique histology, cytogenetic and molecular features.4,5 Using the current WHO classification we recognize subtypes with excellent prognosis (Multilocular cystic renal carcinoma, Type I renal papillary carcinoma, Tubular and spindle cell mucinous carcinoma), from the very aggressive ones (Bellini\\\'s collecting duct carcinoma, Medullary carcinoma).
Despite the incorporation of ever expanding variants of renal carcinoma by the WHO, several independent reports have come forward describing morphological forms not fitting into any of the well known groups6,7 which requires molecular studies and continuous surveillance to determine their exact cellular origin and prognosis.
The aim of this study was to present our data of renal cell carcinoma variants and highlight the importance of correct diagnosis as each type carries its individual prognostic value.
Methods and Results
This study was carried out in the histopathology department of Shifa International Hospital, Islamabad over a period of one and a half year (Jan 2008 to June 2009). Every nephrectomy specimen of renal carcinoma was dealt according to the set protocol8 after adequate fixation. At least three sections were taken from the tumour, one section of renal capsule and painted Gerota\\\'s fascia and one each from renal vein and ureteric resection margin. Sections from remnant renal parenchyma and from pelvis were also submitted. In every specimen a thorough search was made for hilar lymph nodes and adrenal gland. After routine processing, thin sections were obtained and stained with H & E. Each case was diligently examined. Immunohistochemistry (EMA and pan cytokeratin) was also done to confirm the diagnosis in rare variants. Prognostic parameters including tumour size, fuhrman nuclear grade, gerota\\\'s fascial margin, ureteric resection margin, renal vein involvement and pathologic tumour stage were recorded.
During the study period, a total of 13 cases of renal cell carcinoma were diagnosed. Six patients were males while remaining seven were females. The clear cell carcinoma was the most frequent variant (n = 9; 69.2%); with two cases of clear cell carcinoma having more than 50% sarcomatoid component and one case displaying rhabdoid features. There was one case each of chromophobe renal carcinoma (Figure-1),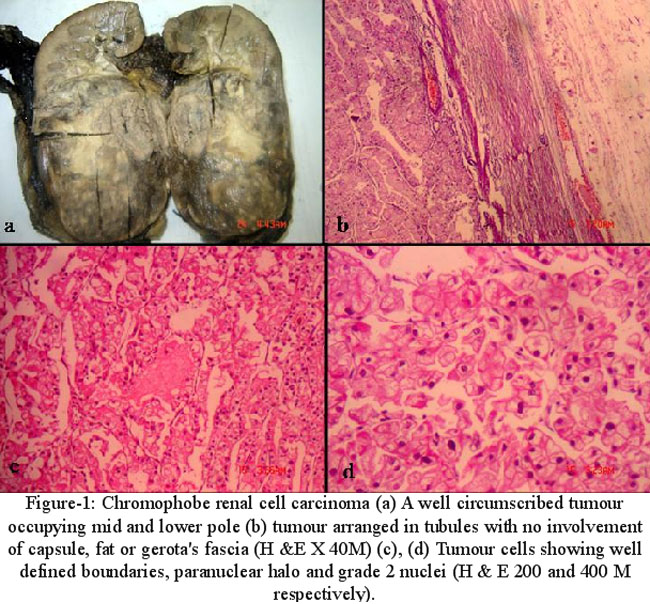
medullary carcinoma, mucinous tubular and spindle cell carcinoma (Figure-2)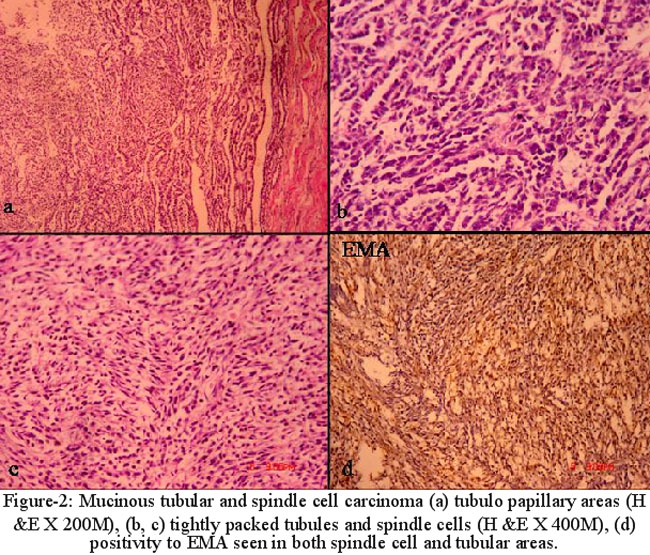
and multilocular cystic renal carcinoma.
The average size of tumour ranged from 2.8 cm to 9.0 cm. Furhman\\\'s nuclear grade 2 was most frequently encountered (n= 6; 46 %). Gerota\\\'s fascial margin, ureteric resection margin and renal vein were free in all cases except two; one being medullary carcinoma and the other clear cell carcinoma with sarcomatoid component. The most frequent pathologic tumour stage was pT2 (n=7; 54%).
Although an attempt was made to gather follow up data, most of the cases were lost to follow up.
Conclusion
Due to an ever expanding spectrum of morphological variants of renal cell carcinoma as well as continuous incorporation of new entities, the recognition of these rarities becomes necessary to reach a correct diagnosis. This case series is limited due to small sample size and the fact that most of the patients were lost to follow up. More such studies on large scale with incorporation of follow up data are recommended to obtain population based statistics and identify biologically favourable variant, which subsequently can steer the therapeutic protocol in future, like less aggressive or nephron sparing surgery.
References
1.Ahmad Z, Azad NS, Yaqoob N, Husain A, Ahsan A, Khan AN, et al. Frequency of primary solid malignant neoplasms in both sexes. As seen in our practice. J Ayub Med Coll Abbottabad 2007; 19: 53-5.
2.Van den Berg E, van der Hout AH, Oosterhuis JW. Cytogenetic analysis of epithelial renal cell tumours: relationship with a new histological classification. Int J Cancer 1993; 55: 223-7.
3.Weiss LM, Gelb AB, Medeiros LJ. Adult renal epithelial neoplasms. Am J Clin Pathol 1995; 103: 624-35.
4.Fleming S. The impact of genetics on the classification of renal carcinoma. Histopathology 1993; 22: 89-92.
5.Kovacs G. Molecular differential pathology of renal cell tumours. Histopathology 1993; 22: 1-8.
6.Amin MB, Michal M, Radhakrishnan A, Hes O, McKenney JK, Cheville JC. Primary thyroid-like follicular carcinoma of the kidney: A histological distinctive primary renal epithelial tumour. Mod Pathol 2004; 17(S1): 136A (A 567).
7.Farah R, Ben-Izhak O, Munichor M, Cohen H. Low-grade renal collecting duct carcinoma. A case report with histochemical, immunohistochemical, and ultrastructural study. Ann Diagn Pathol 2005; 9: 46-8.
8.Eble JN. Recommendations for examining and reporting tumour bearing kidney specimen from adults. Semin Diagn Pathol 1998; 15: 77- 82.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: