
Momen Mohammad Ahmad Almomen ( Medical Student, College of Medicine, Dammam University, Dammam, Saudi Arabia. )
Qusai Loay Abdullah Alsaleh ( Medical Student, College of Medicine, Dammam University, Dammam, Saudi Arabia. )
Ali Mohammad Ahmad Almomen ( Medical Student, College of Medicine, Dammam University, Dammam, Saudi Arabia. )
Ahmed Badar ( Department of Physiology, Dammam University, Dammam, Saudi Arabia. )
January 2011, Volume 61, Issue 1
Student's Corner
Abstract
Objectives: To determine the effect of fasting immediately after exercise on blood lactate clearance.
Methods: This study was conducted at College of Medicine, Dammam University, KSA. Untrained male volunteers (n=26) between 18-23 years of age were divided into two equal groups; fasting and non-fasting. After an overnight fasting both groups were made to exercise on a bicycle ergometer starting with 100 watt resistance with 25 watt increment after every 2 minutes until voluntary exhaustion. The fasting group was then asked to continue fasting 30 minutes after exercise, while the non-fasting group was given 600ml of carbohydrate-rich (about 16g per 100 ml) drink immediately after exercise. We measured the blood lactate level before, immediately after, and 30 minutes after exercise in both the groups.
Results: A significant (p<0.001) increase in mean blood lactate level was observed in both the groups immediately after exercise as compared to the baseline means. Similarly there was a significant (p<0.001) drop of lactate level in both the groups 30 minutes after exercise as compared with the blood lactate level immediately after exercise. There was a significant (p<0.001) difference between the number of subjects with a blood lactate drop of more than 50% between the two groups (84.61% of subjects in the fasting group, versus 46.15% in the non-fasting group).
Conclusion: Fasting after exercise accelerates lactate clearance from blood, probably by utilizing gluconeogenesis pathway.
Keywords: Lactate, Exercise, Fasting (JPMA 61:104; 2011).
Introduction
Energy for skeletal muscle contraction is supplied by both anaerobic and aerobic metabolic pathways. The Anaerobic pathways can allow short bursts of intense physical activity while the aerobic system can sustain physical activity for many hours.1 Carbohydrates are the best fuel for working muscle. The first metabolic pathways of carbohydrate metabolism to be involved are skeletal muscle glycogenolysis and glycolysis. This is followed later on by circulating glucose formed through activated gluconeogenesis. Lactate and amino acids are the major endogenous carbon sources mobilized for the resynthesis of muscle glycogen during recovery from exercise. It has been reported that the capacity of muscles to recover glycogen stores from endogenous carbon sources is dependent on the type of physical activity and animal species.2
Lactate is produced during strenuous exercise by anaerobic glycolysis in the skeletal muscles.3 Massive amounts of lactic acid are produced during endurance sport by muscle cells. This metabolite is thought to be responsible for the muscle pain and fatigue during sport.4 The "maximal lactate steady state" is a measure for the relationship between the highest blood lactate concentration and workload that can be maintained over time without a continual blood lactate accumulation.5 Unlike the previous belief the present understanding is that lactate is formed and utilised continuously under fully aerobic conditions also.6
The lactate formed has two possible fates. A small portion gets converted back into pyruvate and then metabolized oxidatively by all body tissues while a larger portion of it will be converted into glucose.7 The process by which lactate is converted into glucose is called gluconeogenesis in the Cori Cycle. In this cycle, lactate is transferred from the muscles to the liver.3 This process is activated when there is insufficient glucose supply from the diet like during fasting.8
Lactic acid measurement is very important in exercise physiology. It is an indicator of the oxygen debt. The body normally contains about 2 liters of stored oxygen that can be used for aerobic metabolism. In heavy exercise, almost all this stored oxygen is used and then the body moves to the anaerobic threshold where lactic acid is produced. During recovery, two types of oxygen debt have to be paid; first one called "alactacid debt" and the other is called "lactic acid oxygen debt" where the lactic acid produced debt is being paid.7
Muscle fatigue limits the movement of the person after exercise. Many theories have been proposed to explain the cause of fatigue. Intracellular acidosis due mainly to lactic acid accumulation has been regarded as the most important cause of skeletal muscle fatigue. Recent studies on mammalian muscle, however, show little direct effect of acidosis on muscle function at physiological temperatures. Instead, inorganic phosphate, which increases during fatigue due to breakdown of creatine phosphate, appears to be a major cause of muscle fatigue.9
The background of this project was an assumption that if a person takes glucose containing diet immediately after exercise then there is a possibility that lactate stays in blood for a longer time as gluconeogenesis pathway will not be activated due to ample availability of glucose. However if no such diet is used immediately after exercise then most of the lactate will be rapidly cleared by gluconeogenesis. In this study we compared blood lactate clearance between two groups of volunteers; one who took a high glucose drink immediately after strenuous exercise and a group that was kept fasting following an exercise. The objective was to determine effect of fasting immediately after exercise on blood lactate clearance in untrained male volunteers.
Subjects and Methods
This study was carried out at Department of Physiology, College of Medicine, Dammam University, Dammam, Saudi Arabia. Permission for the project was granted by the deanship of Research, Dammam University.
We recruited 26 male, non-trained volunteers aged (18-23) and divided them into 2 equal groups (A & B). Subjects with evidence of liver diseases, kidney diseases, diabetes mellitus, GIT diseases, anaemia, recent musculoskeletal injuries and musculoskeletal diseases were not included. Similarly smokers were not included. An informed consent was taken from all subjects.
Subjects of both groups were asked to fast for 8 hours. When the subjects came to the laboratory, baseline heart rate and blood pressure were recorded. The baseline lactate level (mmol/L) was also determined before the start of exercise.
The subjects were asked to do an incremental exercise on an ergometer bicycle; starting with 100 watt resistance and increasing by 25 watt every 2 minutes until voluntary exhaustion.10
The 2nd estimation of blood lactate level was carried out immediately after the exercise/voluntary exhaustion in both the groups. Also the blood pressure and heart rate were determined immediately after exercise.
Group A (n=13) was given a carbohydrate rich liquid (16 gm/100 ml) in a standard amount (500 ml) immediately after exercise, while Group B (n=13) was kept fasting for 30 minutes. The third blood lactate estimation was carried out after 30 minutes in both the groups. The blood pressure and heart rate were also determined 30 minutes after exercise.
Blood lactate was measured using a hand held device Lactate Scout® (EKF diagnostic, SensLab). This device uses enzymatic-amperometric detection of lactate evaluation. The precision of this method as compared with the conventional methods is recognized.11 The kit provides a standard (12.5 mmol/L) solution to compare results.
The data was analyzed by Statistical Package for Social Sciences (SPSS-14). Mean and standard deviations were calculated for age, heart rate, systolic blood pressure, diastolic blood pressure and lactate. Student "t" test was used to determine significance of differences in lactate levels before and after exercise (immediately after and 30 minutes after) in the same group and between the two groups. Chi square test was used to compare the proportion of subjects with more than 50% drop in serum lactate between the two groups. A \'p\' value of <0.05 was taken as statistically significant.
Results
The mean age of fasting subjects (n=13) was 21.3 ± 0.94 years, while that of non-fasting (n=13) subjects 21.38 ± 0.65 years. The weight of fasting subjects was 69.7 ± 9.72 kg, while that of non-fasting subjects was 67.11 ± 12.34 kg. The height of fasting group was 170.46 ± 3.59 cms while that of non-fasting group was 169.42 ± 6.32 cms. None of the differences was statistically significant reflecting selection of identical controls for paired analysis.
The results of this study are summarized in tables 1-3.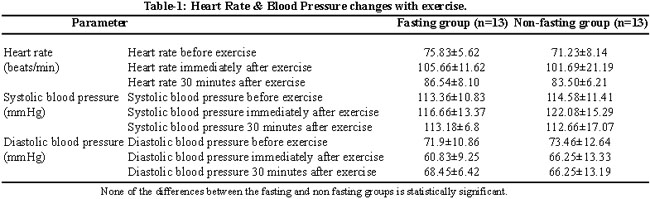
Table-1 shows mean heart rate before exercise, immediately after exercise and 30 minutes after exercise in both the groups. This table also gives mean systolic and diastolic blood pressures before, immediately after and 30 minutes after the exercise for both the groups. None of these was significantly different between the fasting and non fasting groups.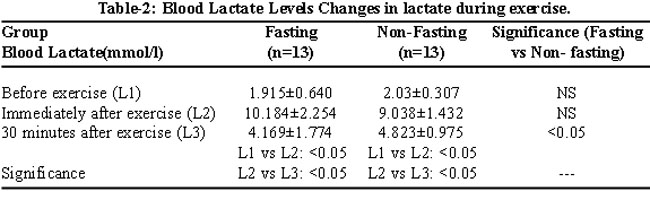
Table-2 shows blood lactate level before exercise (L1), immediately after exercise (L2) and 30 minutes after exercise (L3) for both the groups while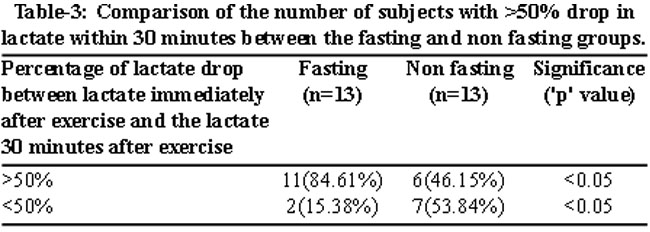
table-3 gives a comparison of subjects with more than 50 % fall in blood lactate level within 30 minutes between the fasting and non fasting groups.
Discussion
Numerous studies have shown that ingesting carbohydrate in the form of a drink can improve exercise performance by maintaining blood glucose levels and sparing endogenous glycogen stores.12 Carbohydrate replacement during exercise may enhance performance of sports and activities, which typically deplete body carbohydrate stores, by providing an additional fuel source for the muscle.13
Reduction of body stores of carbohydrate and blood glucose is related to the perception of fatigue and the inability to maintain high-quality performance. General consensus is that prevention of carbohydrate depletion begins with a high-carbohydrate training diet of about 60-70% carbohydrate, carbohydrate beverages during the event to reduce the chance of body carbohydrate depletion and finally, replacement of body carbohydrate stores rapidly by 40-60 g of carbohydrate consumption as soon as possible after the exercise and repeating 1-hourly intervals for at least 5 hours after the event.14
With this background most of the studies in available literature mention positive effects of carbohydrate rich diet and supplements on endurance and performance of athletes. Very few have addressed the effect of carbohydrate supplementation after or during exercise on fatigue or on lactate. Our hypothesis was totally different from the accepted norms as we tried to look into possible delay of lactate clearance due to ample glucose availability in people ingesting high carbohydrate diet before, during or after exercise. We determined the effect of fasting and continued fasting on blood lactate level. We observed that following a post-exercise rise blood lactate returned towards the baseline value more quickly in more subjects in the fasting group.
A study carried out in India to determine the effect of carbohydrate-electrolyte drink on blood lactate levels during exercise and recovery, supports our results. It noted that supplementation of 5 g per cent carbohydrate-electrolyte drink keeps the blood lactate at lower levels. This study showed that removal of blood lactate was significantly (P<0.05) faster after 10 min (without supplementation 3.1±1.0 mmol/l; with supplementation 2.1±0.8 mmol/l) and 20 min (without supplementation 2.5 ± 0.9 mmol/l; with supplementation 1.5±0.4 mmol/l) with 12.5 g per cent carbohydrate-electrolyte drink.13
Lactate has been proposed as a cause of muscle fatigue in some references, others attribute it to other causes such as inorganic phosphate, which increases during fatigue due to breakdown of creatine phosphate.9 There is a controversy about the percentage of the lactate being converted into glucose by the process of gluconeogenesis. Some say that 50% of lactate is converted to glucose.10 Others say that 20% of lactate is converted to glucose.15 If we assume that the lactate is a cause of muscle fatigue, we would say that increasing the removal rate of the lactate would help us in the process of the recovery from muscle fatigue.
Among glucose metabolites, lactate plays a primary role as either direct or indirect (gluconeogenesis) energy source for contracting skeletal muscle.1 Studies have shown that gluconeogenesis capacity is available in humans after an overnight fast and can be used to sustain blood glucose levels during low-intensity exercise when lactate is available at elevated plasma levels.16
Internal removal of lactate from the body by enzymatic conversion depends mainly on the capacity of the hepatic gluconeogenesis that converts lactic acid to glucose.4 Lactate disposal is mainly through oxidation, especially during exercise when oxidation accounts for 70-75% of removal and gluconeogenesis for the remainder.6
Roaef et al studied the role of lactate in gluconeogenesis during exercise in untrained fasting humans. They reported that exercise induced a decrease in blood glucose concentration from 5.0 +/- 0.2 to 4.2 +/- 0.3 mM (P < 0.05); lactate infusion abolished this decrease (5.0 +/- 0.3 mM; P < 0.001) and increased glucose. They concluded that that lactate infusion during low-intensity exercise in fasting humans increases gluconeogenesis from lactate and increased glucose production, thus increasing the blood glucose concentration.16
The main limitation of our study was that we did not measure glucose level and pH along with lactate, therefore we will recommend further studies to work out this important aspect of delayed or hindered lactate clearance due to high availability of glucose in athletes using carbohydrate supplements before, during and after exercise.
Conclusion
Fasting after exercise accelerates lactate clearance from blood, probably by utilizing gluconeogenesis pathway.
References
1.De Feo P, Di Loreto C, Lucidi P, Murdolo G, Parlanti N, De Cicco A, et al. Metabolic response to exercise. J Endocrinol Invest 2003; 26: 851-4.
2.Fournier PA, Bräu L, Ferreira LD, Fairchild T, Raja G, James A, et al. Glycogen resynthesis in the absence of food ingestion during recovery from moderate or high intensity physical activity: novel insights from rat and human studies. Comp Biochem Physiol A Mol Integr Physiol 2002; 133: 755-63.
3.Haris RA. Carbohydrate Metabolism I: Major metabolic pathways and their control. In: Devilen TM, editors. Textbook of biochemistry with clinical correlation. 5th ed New York : Wiley-Liss 2002; pp 598-663
4.Bongaerts GP, Wagener DJ. Increased hepatic gluconeogenesis: the secret of Lance Armstrong\'s success. Med Hypotheses 2007; 68: 9-11.
5.Billat VL, Sirvent P, Py G, Koralsztein JP, Mercier J. The concept of maximal lactate steady state: a bridge between biochemistry, physiology and sport science. Sports Med. 2003; 33: 407-26.
6.Brooks GA. Lactate: link between glycolytic and oxidative metabolism. Sports Med 2007; 37: 341-3.
7.Guyton AC, Hall JE. Textbook of Medical Physiology. 11th ed. Philadelphia: Pennsylvania; Elseviers Saunders, 2006.
8.Mayes PA. Gluconeogenesis and Control of the blood glucose. In: Murray RK, Rodwell VW, Bender D, Botham KM, Weil PA, Kennelly PJ. Harper\'s Illustrated Biochemistry. 28th ed. Norwalk: McGraw-Hill, 2009; pp 191-221.
9.Westerblad H, Allen DG, Lännergren J. Muscle fatigue: lactic acid or inorganic phosphate the major cause? News Physiol Sci 2002; 17: 17-21.
10.Astrand PO, Hultman E, Juhlin-Dannfelt A, Reynolds G. Disposal of lactate during and after strenuous exercise in humans. J Appl Physiol 1986; 61: 338-43.
11.Ferasin L, Dodkin SJ Amodio A, Murray JK, Papasouliotis K. Evaluation of a portable lactate analyzer (Lactate Scout) in dogs. Veterinary Clin Pathol 2008; 36: 36-9.
12.Campbell C, Prince D, Braun M, Applegate E, Casazza GA.Carbohydrate-supplement form and exercise performance. Int J Sport Nutr Exerc Metab 2008; 18: 179-90.
13.Khanna GL, Manna I. Supplementary effect of carbohydrate-electrolyte drink on sports performance, lactate removal & cardiovascular response of athletes. Indian J Med Res 2005; 121: 665-9.
14.Walberg-Rankin J. Dietary carbohydrate as an ergogenic aid for prolonged and brief competitions in sport. Int J Sport Nutr 1995; 5 Suppl: S13-28.
15.Lindinger MI. Lactic acid accumulation is an advantage/disadvantage during muscle activity. J Appl Physiol 2006; 100: 2100-2.
16.Roef MJ, de Meer K, Kalhan SC, Straver H, Berger R, Reijngoud DJ. Gluconeogenesis in humans with induced hyperlactatemia during low-intensity exercise. Am J Physiol Endocrinol Metab 2003; 284: E1162-71.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: