
Suneel Kumar Punjabi ( LUMHS, Jamshoro, Karachi. )
Habib-ur-Rehman ( Department of Oral & Maxillofacial Surgery, Abbasi Shaheed Hospital, Karachi. )
Zahid Ali ( Department of Oral & Maxillofacial Surgery, Abbasi Shaheed Hospital, Karachi. )
Shaheen Ahmed ( Department of Oral & Maxillofacial Surgery, Abbasi Shaheed Hospital, Karachi. )
January 2011, Volume 61, Issue 1
Original Article
Abstract
Objectives: To assess the causes and management of Zygomatic bone fractures at Abbasi Shaheed Hospital, Karachi.
Methods: This study was carried out at Department of Oral & Maxillofacial surgery Abbasi Shaheed Hospital, Karachi. A total of 82 cases were studied. A detailed history was taken, clinical examination was performed and fractures were confirmed by radiography. Management of fractures was done by using different proposed modalities, suitable for every case. A number of factors, like age of patients, causes of trauma and gender were assessed.
Results: The commonest cause of Zygomatic bone fracture was found to be road traffic accident (RTA) 50% (n=41), followed by assault 23.17% (n=19) , fall 20.73% (n=17) , sports injuries 3.65% (n=3), and others 2.43% (n=2) respectively. Right side (55%) was involved a little more than the left side (45%).
Zygomatic bone fracture was more prevalent in age group between 21-30 years, while male to female ratio was 5.30:1. Remote reduction using Gillie\'s Temporal Approach with and without fixation using bone plates were the commonest management modalities used in this center.
Conclusion: The commonest cause of Zygomatic bone fracture was found to be road traffic accident, with the right side fractures being more common. It reveals poor road traffic sense in road users, lack of road safety measures and legislation in our population.
Keywords: Zygomatic bone fractures, Road Traffic Accident, Assault, Gillies temporal approach, Bone plates (JPMA 61:36; 2011).
Introduction
Zygomatic or Malar bone fractures are second after nasal bone fractures among facial skeletal injures.1,2 The high incidence of these fractures may probably be attributed to the fact that Zygoma\'s occupy an anatomically prominent position within the facial skeleton3 which frequently exposes it to traumatic forces. The Zygoma is roughly quadrilateral in shape, with an outer convex surface and an inner concave surface. The convexity forms the point of greatest prominence of the cheek; therefore the Zygoma plays a major role in facial contour, and disruption of Zygomatic bone carries a risk of functional and aesthetic impairment.4,5 The characteristic sign and striking feature of Zygomatic fracture is flattening of the normal prominence, lip sag and limitation of mouth opening.6,7 Etiology in facial trauma is not different from the trauma in other body regions, although due to delicate but compact anatomy, the results are more devastating in facial region. In western countries, inter personal violence is the commonest cause,2 whereas in developing countries road traffic accidents result with more facial trauma than any other cause.4 Other causes of the facial trauma include industrial, accidentals, sports injuries, falls and FAI (Fire Arm Injry).8,9
The relative importance of the various factors, which affect the incidence of facial bone fractures, is influenced by geography, social trends, alcohol and drug abuse.
The etiology of maxillofacial injuries varies from state to state and it shows that some of the variations can be attributed to social, cultural and environmental factors.2
According to statistics of World Health Organization (WHO) more than 1 million people die and around 15 to 20 million people are traumatized in road traffic accident annually.10 Moreover, there were 15390 estimated cases of facial bone fractures in England and Wales in six years, out of which 50% of fractures of the face involved the fracture of the Zygomatic bone.11
Since the shape of the face is influenced greatly by the underlying osseous structure, the Zygoma plays an important role in the facial contour. Therefore, for both cosmetic and functional reasons, it is important that Zygomatic fractures should be properly diagnosed and suitably treated. The treatment modalities of Zygomatic bone fracture vary, depending mostly upon displacement of fractures and stability after reduction. There are several techniques for the reduction of the fractured Zygomatic bone including closed reduction like Gillies temporal approach,12 percutaneous hook and open reduction. Fixation of unstable fractures is done with Transosseous wires or bone plates.
The common age group and causes of Zygomatic bone fracture in this part of country are also mentioned in this study. This study may provide evidence for recommendation of possible preventive measures, keeping the etiology in view. For example, the introduction of seat belt legislation in developed countries, as expected led to a remarkable fall in the number of maxillofacial injuries (including Zygomatic bone fractures) from road traffic accident.
Patients and Methods
The study was carried out at the Oral and Maxillofacial Surgery Department of Abbasi Shaheed Hospital Karachi, which is a tertiary care hospital with a catchment population of more than 2 million people.
A total of 82 patients who attended the OPD or Emergency department from 1st Jan 2007 to 31st Dec 2008, were studied for the causes and management of Zygomatic bone fractures.
A comprehensive history was taken, at least two radiographs were assessed using the clinical information by the team of researchers consisting of an assistant professor, and two senior residents and a junior resident of oral and maxillofacial surgery department.
A written informed consent was obtained from the patient or attendant, and questionnaire filled for each patient for factors like, age, gender, and cause of injury. Properly filled questionnaires were used to record and compile the study data. The treatment of fractures was done by standard methods of reduction and fixation. Reduction was done by Gillies Temporal Approach, or Percutaneous Bone Hook technique.
Fixation was done for unstable fractures after reduction, using Bone Plates, or Transosseous Wiring.
Patients from any age group or gender with clinically evident signs and symptoms and radiological evidence of Zygomatic bone fracture were included in the study.
Whereas patients who were medically compromised previously maltreated or untreated or with other associated facial skeletal fractures were excluded from the study.
Data was analyzed in statistical programme for social sciences (SPSS) version 11.0. The frequency and percentage was computed for qualitative variables, like gender, etiologies, pattern and management modalities. Mean± standard deviation was computed for qualitative variables, like age.
No inferential test was applied due to descriptive statistics.
Results
The results of this study were described in sequence of the objectives.
Detailed description of separate results is shown as follows.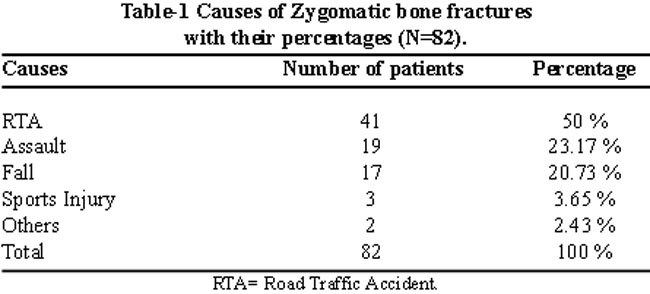
Table-1 shows the causes of the Zygomatic bone fracture.
The pattern of Zygomatic bone fractures resulted in right side predominance with 57.31 % (n=47) while left side was involved in 42.68 % (n=35).
Management of Zygomatic bone fractures was carried out by different modalities as found suitable for individual fracture and patient. The total number of different management technique used is tabulated and sorted separately for the frequency of each type. Results are described in Table-2.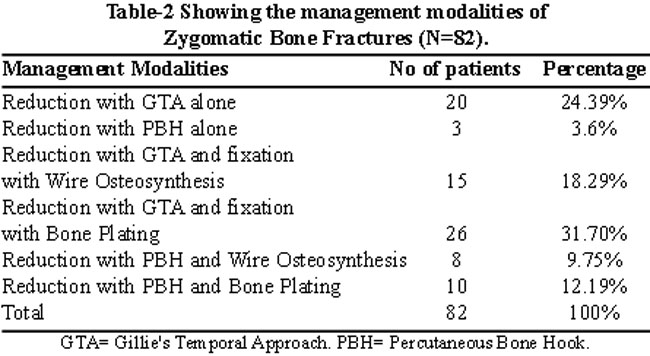
Gender distribution shows male predominance with males being 84.14 % (n=69) and females being 15.85 % (n=13).
Age distribution of patients of Zygomatic bone fracture shows third decade to be most common followed by fourth decade. Notably there were no cases recorded in the first decade of life. The age distribution is shown in Table-3.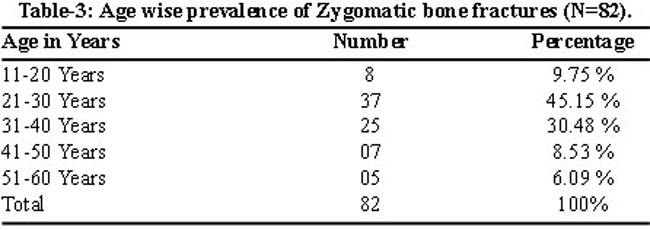
Discussion
This is a local study utilizing the residents of a metropolitan city. Gender distribution of the reported Zygomatic bone fractures describe that 84.14% (n=69) patients were males, and 15.85 % (n=13) were females. This 5.30:1 ratio of male preponderance can be explained by the fact that the majority of such fractures result from road traffic accidents, assault, falls, sports injuries etc. where men are more commonly involved. This ratio is comparable to similar studies done in other countries.4,8,13,14 However remarkable increased ratio of males in this study population, indicates that males are more involved in outdoor activities. The low ratio of females in this study may be, due to the socio-religious reasons where females are relatively inactive in outdoor activities.
The predominant age group in this study was 21 to 30 years that is also similar to other studies8,9,13,15-18 done in other ethnic groups. The young adult is more actively involved in outdoor activities during this phase of life e.g. social activities, business and sports, high speed transportation, which makes them more vulnerable to the fracture under study.
The causes of maxillofacial injuries have changed over the last three to four decades and they are expected to continue.19 The contemporary cases of the fracture of the facial bones are in order of frequency; interpersonal violence, sporting injuries, falls and road traffic accidents. More recently this changing pattern of maxillofacial injuries has been reviewed by Van Beak and Markx,20 who have compared their own longitudinal studies from the Netherlands with similar data from Hamburg and Great Britain. The developed countries all show a striking reduction in the broad category of road traffic accidents and the increasing influence of interpersonal violence.20 This was not the case in this study where road traffic accident was by far the most common cause of Zygomatic bone fractures (50%), and assault accounts for only (23.17%) of total 82 cases. These results are more compatible with results of a local study done by Noorul Wahab et al4 who assessed the etiology of Zygomatic bone fractures in another city, Lahore of the same country and stated that the most common cause of ZMC fractures was road traffic accident (RTA) 52.5%(n=21), followed by fall 17.5% (n=7), fire arm injury (FAI) 15%(n=6), interpersonal violence (IPV) 7.5%(n=3), occupational trauma and sport injuries 5%(n=2) and 2.5%(n=1) respectively. Another local study done by Qayyum Z et al7 utilizing the population of capital city of Pakistan also described the same ratio and relevance of etiology. Their results show road traffic accident as the most common cause of ZMC fractures followed by fall, fire arm injury (FAI), interpersonal violence (IPV), occupational trauma and sport injuries. This also demonstrates that the causes of maxillofacial injuries depend on, social, cultural and geographic system.
The high figure of maxillofacial injuries due to road traffic accidents in Pakistan is due to the lack of road sense among the road users, poor condition of vehicles and roads and poor compliance with transportation regulations. Most of the people in this region of the country belong to a low socio-economic status, compelled to use public transport vehicles, driven by illiterate, devoid of road sense, negligent and under-age drivers. All stated factors co-operate to make road traffic accidents the leading cause of maxillofacial and Zygomatic bone fractures in this part of world.
The assault is a common cause of trauma in most developed and under developed countries. It is due to alcohol and drug abuse, illiteracy and social frustration. The incidence of assault in the study was found to be 23.17 %. The same results were reported by Gusztav from U.A.E. and Haider;9 from Jordan. Alcohol intake is usually a contributing factor to both assaults21 and RTA19 in European countries. Fall was the third most common cause of Zygomatic bone fractures in this study being 20.73%. Fall, as an etiological factor, is comparable to the previous studies,22 but it is slightly low in this study population than others.2,21 Sports related fractures are becoming increasingly common due to a growing interest in the sports activities throughout the world. Some researchers show sports related Zygomatic bone fractures as high as 8.8%2,23 but a lower incidence of only 3.65% was observed in this study. Reason for this low result maybe lack of sports and recreation facilities, and low socioeconomic status, in this region. This study results are similar to the previous findings that most of the fractures are unilateral.7,11
In this study (100%) Zygomatic bone fractures were unilateral. Right side was mostly involved. Same results were reported by a previous study in India. Injury to the left side of the face showed more predominance in the cases of trauma due to assaults.10 This may be due to the fact that majority of the population is right handed. Similar findings were observed in this study.
Management of Zygomatic bone fractures are discussed and compared by many authorities in different parts of world.10 Many have suggested the management of fractured Zygomatic bone by distant or direct reduction only, without fixation by any means. While many others have advocated reduction and fixation of the fractured parts of Zygomatic bone with bone plating or wire Osteosynthesis. All reasons given to favour their statements are valid, as it depends upon the type of fracture, availability of hardware and proficiency of the operating surgeon. If the conditions are favourable, the results of reduction and fixation with bone plating are higher than any other modality. Wu H, Zhu Z and Li Y also support this statement by reporting that mini bone plates fixation for mid face fractures is more convenient and reliable than wire Osteosynthesis.24
Conclusion
The results of this study show, that road traffic accident is the most common cause of Zygomatic bone fractures in this part of the country. The reason for this is that there is lack of road sense amongst road user, poor condition of the vehicles and roads and increased traffic load. There is clear need of educating the road users about the protection measures and necessary seat belt and helmet legislation enforcement, which will decrease the numbers of maxillofacial injuries including isolated Zygomatic bone fractures in developed countries. The most common age group in this study was from 21-30 years, which shows that this period is most active part of life when people get involved in daring activities.
References
1.Hollows P, D\'Sa A, McAndrew PG. Life-threatening heamorrhage after elevation of a fractured zygoma. Br J Oral Maxillofac Surg 1999; 37: 448-50.
2.Israr N, Shah AA. Retrospective study of zygomatic complex fractures in Sheffield England. Pak Oral Dent J 2001; 21:50-9.
3.Strong EB, Sykes JM. Zygoma compex fracture. Facial Plast Surg 1998; 14: 105-15.
4.Wahab N, Mehdi H, Khan M. Causes of Zygomatic bone fracture reported at Mayo Hospital, Lahore. J Pak Dent Assoc.2008; 17: 31-4.
5.Lee KH, Antoun J. Zygomatic fractures presenting to a tertiary trauma centre, 1996-2006. N Z Dent J 2009; 105: 4-7.
6.Ellis E III. Fracture of the Zygomatic complex and arch. In; Fonsca RJ, walker RV, editors. Oral and Maxillofacial trauma. 2nd ed. Philadelphia: WB Saunders; 1997; pp 571-632.
7.Qayyum Z, Khitab U. Normal range of mouth opening in adults. Pak Oral Dent J 2002; 22: 147-48.
8.Zachariades N, Papavssilliou D. The pattern and etiology of maxillofacial injuries in Greece: A retrospective study of 25 years and a comparison with other countries. J Cranio Maxfac Surg 1990; 18: 251-4.
9.Haider Z. Fracture of the Zygomatic complex in the south east region of Scotland. Br J Oral Surg 1997; 15: 265.
10.Schnetler JF. A technique for reducing fractures of the zygomatic complex under local anesthesia.Br J Oral Maxillofac Surg 1990; 28: 168-71.
11.Courtney DJ. Upper buccal sulcus approach to management of fractures of the zygomatic complex: a retrospective study of 50 cases. Br J Oral Maxillofac Surg 1999; 37: 464-8.
12.Sullwain WG, Richard J. Fracture of the Zygoma in: Cohen on editor. Master of plastic and reconstructive surgery. 1st ed. New York; Little Brown and company; 1994.
13.Adekeye EO. The pattern of fractures of the facial skeleton in kaduna, Nigeria. A survey of 1447 cases. Oral Surg Oral Med Oral Pathol 1980; 49: 491-5.
14.WHO Statistics Annual 1992. WHO: Geneva, 1992.
15.Adekeye EO, Fractures of the zygomatic complex in Nigerian patients. J Oral Surg 1980; 38: 596-9.
16.Shepherd JP, Irish M, Scullye C, Leslie. Alcohol intoxication and severity of injury in assault. Br Med J 1988; 296: 1299-303.
17.Afzelivs LE, Rosen C. Facial fractures. A review of 368 cases. Int J Oral Surg 1980; 9: 25-32.
18.Starkhammer H, Olofsson J. Facial fracture. A review of 922 cases with special reference to incidence and aetiology. Clin Otolaryngol 1982; 7: 405-9.
19.Tanaka ON, Tomitsuka K, Shionoya K, Andou H , Kiimijima Y, Tashiro T, et al. Aetiology of maxillofacial fractures. Br J Oral Maxillofac Surg 1994; 32: 19-23.
20.Van beek Gj, Merkx CA. Changes in the pattern of fratures of the maxillofacial skeleton. Int J Oral Maxillofac Surg 1999; 28: 424-8.
21.Torgerson M, Tornes k. Maxillofacial fractures in norwgial district. Int J Oral Maxillofac Surg 1992; 21: 335-8.
22.Qiam D. Analysis of 362 cases of maxillofacial injuries in northern region of Pakistan. Pak Oral Dent J 1991; 11: 35-43.
23.Cook HE, Row M. A retrospective study of 356 midfacial fractures occurring in 225 patients. J Oral Maxillofac Surg 1990; 48: 574-8.
24.Wu H, Zhu Z, Li Y. Comparison of internal fixation with mini-titanium plate and wire osteosynthesis in midface fractures. Zhonghua Zheng Xing Shao Shang Wai Ke Za Zhi 1999; 15: 120-2.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: