
Shahid Wahab ( Department of Ophthalmology, Sindh Govt. Lyari General Hospital, Karachi. )
Jamshed Ahmed ( Department of Ophthalmology, Dow University of Health Sciences, Karachi. )
Khwaja Sharif-ul-Hasan ( Department of Ophthalmology, Baqai Medical University Hospital, Karachi. )
January 2011, Volume 61, Issue 1
Original Article
Abstract
Objective: To evaluate the safety and efficacy of pars plana surgical posterior capsulotomy in pseudophakic adults.
Methods: This prospective interventional case series was conducted at Sindh Govt Lyari General Hospital Karachi and Al- Noor Eye Hospital Karachi from June 2006 to May 2008. Complete ophthalmic examination of anterior and posterior segment was performed including assessment of type of posterior capsular opacification, measurement of intraocular pressure. Visual acuity, measurement of intraocular pressure and any unwanted complications were analyzed.
Results: Seventy six (43.18%) patients were operated on both eyes. Mean age was 62.01 ± 13.02 years. There were 104(59.1%) females and 72(40.9%) males. Visual acuity at presentation was found to be 6/9 to 6/18 in 130(59.1%)eyes, 6/18 to 6/60 in 81(36.8%) and below 6/60 in 9 (4.1%) eyes. A significant reduction in intraocular pressure (13.8, ± 1.4, P=0.000) was noted on second post operative day. Intraoperative complication included subconjuctival haemorrhage in 22(10%) eyes, pin head haematoma at the entry site in 7(3.2%) eyes, pea head haematoma at the entry site in 8(3.6%) eyes, minor grade of vitreous haemorrhage in 9(4.1%) cases. Insufficient capsular opening was noted in 8(3.6%) eyes. Clinically evident macular oedema in 4(1.8%) eyes. We found no case of endophthalmitis or retinal detachment.
Conclusion: Surgical posterior capsulotomy is a safe and effective procedure in experienced hands and could be adopted in place of YAG laser.
Keywords: Pars plana surgical capsulotomy, Intraocular pressure, subconjunctival haemorrhage, pin head haematoma, peahead haematoma, YAG laser (JPMA 61:14; 2011).
Introduction
Thousands of cataract surgeries with implantation of intraocular lenses are being done in eye camps of which approximately half of them become blind or visually impaired due to Posterior Capsular Opacification (PCO) as one of the major cause.1,2 This is due to fact that YAG Laser is not available at eye camps. Surgeons operate and they never go back again to address PCO. Incidence of PCO is high in eye camps because of high incidence of retained lens materials, inflammation and improper medication.3
Substandard lenses costing less than $5.00 further aggravate this problem.4 The best answer till today is YAG laser posterior capsulotomy. The YAG procedure is a very destructive procedure but is the only best procedure available till today. During YAG laser capsulotomy, micro explosions are produced in a minute space, there is development of shock waves and production of heat up to 10,000 degrees centigrade.5 When the intensity of light propagating in a transparent medium is sufficiently high, atoms are ionized. This is called laser induced breakdown or optical breakdown. By ionization plasma is formed, this is a fourth state of the matter. Plasma absorbs heat termed as "plasma shielding effect." 6 FDA reported that damage to the optic or haptics of an intraocular lens may release substances potentially toxic to intraocular tissues.7 Prevalence of IOL damage has been reported as being between 40% to 81%.8 In addition protocol for performing YAG laser, as described elsewhere9 is not strictly followed.
In the past any intervention through pars plana was only practiced by the vitreo -retinal surgeons but at present after the invention of anti vascular endothelial growth factors (VEGF) many anterior segment surgeons feel comfortable to enter the vitreous cavity through pars plana.10 Keeping all these facts in mind what is the role of surgical capsulotomy?
Surgical capsulotomy can be done in eye camps, in small towns / cities where YAG is not available, in big cities where patient cannot afford the cost of YAG laser. We need to change the attitude for appropriate technology for our need and resources. If the patient cannot sit still or fixate on slit lamp being too old or too young, this procedure is the only choice.
We do not find any details in textbooks for this procedure. There is still a need for it in our society and circumstances (developing and under developed countries).
This study was therefore undertaken to assess the safety of pars plana posterior capsulotomy in pseudophakik adults.
Patients and Methods
All the patient above the age of thirty years with a diagnosis of PCO and willing to participate in the study were selected from out patients department of Sindh Govt. Lyari General Hospital Karachi and Al- Noor Eye Hospital Karachi from June 2006 to May 2008.
The exclusion criteria were: Patients with ARMD, Diabetic maculopathy, Uncontrolled glaucoma and those with Corneal opacity likely to reduce vision.
After taking informed consent, socio-demographic data was recorded and patients were inquired about duration since cataract surgery, type of intraocular lens implanted, place of surgery, drugs used after surgery. Visual acuity was recorded by using Snellen\'s chart. All the patients underwent complete ophthalmic examination with full pupillary dilatation on a biomicroscope. PCO was graded according to the following method as described by Aslam and Patton:11
Grade 0: None visible at all
Grade 1: Visible but none reaching to IOL edge
Grade 2: At IOL edge
Grade 3: Well Inside IOL edge but visual axis clear
Grade 4: Across visual axis.
In addition to grading, type of PCO was documented as capsular fibrosois , Elschnig\'s pearls, combined and capsular wrinkling. Intraocular pressure was recorded by Goldman applanation tonometer. Posterior segment was examined by indirect ophthalmoscope and +90 D to exclude posterior segment pathologies in patients where media was clear to allow this.
Surgical capsulotomy was performed by principal author, a vitreoretinal surgeon by using topical Anaesthesia. Opsite was applied to the eye and conjunctiva was washed with 5% povidone iodine solution. A 27G needle was passed perpendicularly through temporal or nasal Pars Plana 3.0 mm behind the corneoscleral limbus with sliding of the conjuctiva to avoid overlapping entry with counterfixation on opposite side using a Collibri Fixation forcep. Optimum care was taken to have single entry to avoid softenting of the eye. Needle was advanced until it touched the optical edge of the IOL and then slipped between the optical edge and the posterior capsule. Posterior capsule was engaged in the tip of the needle, upward and downwards movements in the plane of the capsule were performed making scleral entrance as the fulcrum for movement with counter pressure applied with collibri forcep. When a small opening was made it was enlarged by horizontal movement of the needle with one of the entering edge of the needle faced posteriorly. Majority of the time single engagement and slight movement achived the objective. Before withdrawal of needele out of the sclera, conjuctiva around the needle was pinched with collibri forcep and needle taken out.
After the procedure the eye was padded for two hours to avoid damage due to undue rubbing( suface anaesthesia) and photophobia induced by the dilating drops. Patients were advised to remove the dressing themselves. Patients were given topical broad spectrum antibiotics Ciprofloxacin four hourly for three days and topical dexamethasone six hourly for three days or combination therapy.
Patients were followed on the next day and then after one week to record best corrected visual acuity. Topical non steroidal anti inflammatory drops were applied in cases where macular oedema was suspected.
Data was entered and analyzed on SPSS version 15 for windows. Decimal notation of Snellen\'s visual acuity was used for statistical analysis. Frequency distribution tables were used to present the data. Mean and standard deviation were used for continuous variables. Categorical variables were presented as proportions and percentages. Paired t-test was used to test the significance before and after surgical capsulotomy at an alpha value of 0.05.
Results
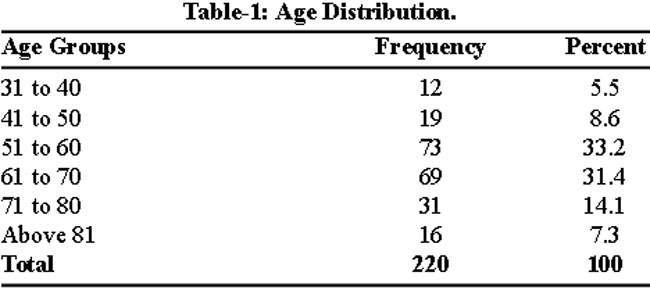
A total of 220 eyes of 176 patients underwent surgical posterior capsulotomy. Seventy six (43.18%) patients were operated on both eyes while 62 (29.54%) on the right eye and 48(27.27%) on the left eye. Mean age was 62.01 ± 13.02 years. The age distribution of the patients is shown in Table-1.
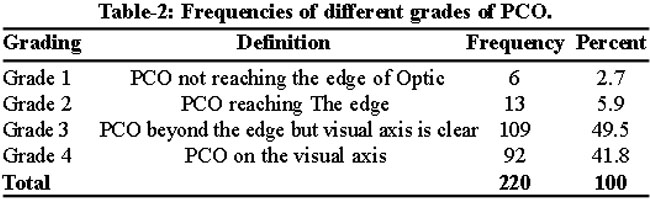
There were 104(59.1%) females and 72(40.9%) males. Mean duration from cataract surgery to the capsulotomy was 21.19 ± 18.7 months which ranged from 3 months to 67 months. Slit lamp examination revealed capsular fibrosis in 121(55%) eyes, Elschnig's pearls in 77(35%) eyes, combined fibrosis and pearls in 11(5%) eyes and capsular wrinkling as a cause of decreased vision in 11(5%) eyes. The grading of PCO can be seen in Table-2.
All the patients presented with decreased vision. Visual acuity at presentation was found to be 6/9 to 6/18 in 130(59.1%) eyes, from 6/24 to 6/60 in 79(35.9%) and below 6/60 in 9 (4.1%) eyes. After surgical capsulotomy visual acuity improved 6/6 in 211(95.9%) cases. Mean intraocular pressure before surgery was 14.8 ± 1.7 mm Hg. Raised intraocular pressure up to five mm. Hg was noted in 16(7.27%) patients on first postoperative day. None of the patients crossed upper limit of normal intraocular pressure. All these returned to preoperative level after 6 weeks. Intraoperative complications encountered are shown in Table-3.
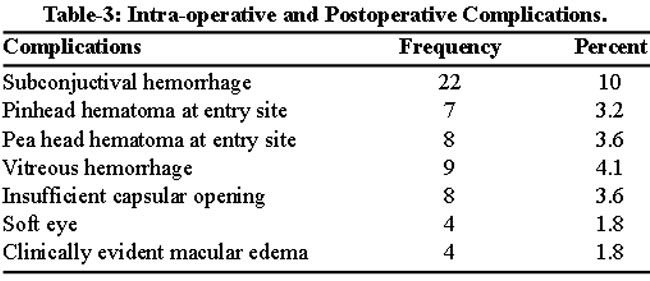
All these complication resolved in 3 to 4 weeks duration. Insufficient capsular opening was noted in 8(3.6%) eyes, which subsequently enlarged due to capsular retraction over two weeks time. Clinically evident macular oedema developed in 4(1.8%) eyes, which resolved over 6 weeks period after local application of non-steroidal anti-inflammatory drops. No case of endophthalmitis or retinal detachment was reported until last follow up (one year).
Discussion
Developing countries have an enormous burden of cataract surgery. A large number of surgeries are performed in eye camps and in hospitals funded by non-governmental organizations where a surgeon has to operate on dozens of cases in a short time. As a result in many cases lens matter is not completely cleaned which leads to posterior capsular opacification. Normally about 25 percent patients over a period of five years develop visually significant posterior capsular opacification.12 Neodymium YAG laser posterior capsulotomy is not available in remote areas where camp surgery is performed to address the problem of blindness and visual impairment related to posterior capsular opacification. To overcome this problem an alternate method has to be adopted which is time and money saving and easy to perform in an ordinary surgical setup. Surgical capsulotomy could solve all these problems if performed by a well-trained surgeon under all aseptic measures. In our series of 220 cases who underwent surgical capsulotomy through pars plana there was no sight threatening complication like endophthalmitis and retinal detachment. Ambler and Constable in a series of 862 cases reported 1.4% incidence of retinal detachment after YAG Laser posterior capsulotomy within 6 months after the procedure.13 Paivi et al in a cohort of 350 eyes over a period of five years reported 2.0% incidence of retinal detachment.14 In our study we followed these patients for only one year with no incidence of retinal detachment. Leonard et al in 1992 performed surgical Capsulotomy by an open chamber technique in 587 eyes (51 aphakic and 536 pseudophakic).15 They reported three cases of endophthalmitis, one case of serious eye damage due to retro-bulbar anaesthesia, two cases of marked elevation of intra ocular pressure and nine cases of retinal detachment. We adopted a closed chamber technique without retro-bulbar anaesthesia. In their series raised intraocular pressure was observed in one aphakic eye due to pupillary block by the vitreous and in the other eye due to retained viscoelastic material. In our series we excluded aphakic eyes and did not use any viscoelastic material. Endophthalmitis reported in Leonard’s series could be due to inadequate sterilization and non-availability of broad spectrum antibiotics in that era. Retinal detachment could be avoided if these kinds of operations are performed by a surgeon who has a sound knowledge of posterior segment. Nowadays anti VEGF are being widely used with minimum side effects if done in a correct manner. In the beginning complication rates were high after anti VEGF injection but nowadays strictly following proper protocols have made these procedure safe. It is observed that the learning curve is steep for this type of capsulotomies. It is easy for a surgeon who has mastered capsulorrhexis. Confidence in handling the anterior capsule gives an edge to handle the posterior capsule. Surgical capsulotomies are cost effective, can be performed in lying position and there is no danger of lens pitting retinal detachment and increased intraocular pressure.
Conclusion
Surgical posterior capsulotomy is a safe and effective procedure in experienced hands and could be adopted in place of YAG laser. We should formulate a protocol for surgical capsulotomy so that this procedure could be preformed in a scientific way without any avoidable complication.
References
1.Kapoor H, Chatterjee A, Daniel R, Foster A.Evaluation of visual outcome of cataract surgery in an Indian eye camp. Br J Ophthalmol 1999; 83: 343-6.
2.Shrestha J K, Pradhan Y M and Snellingen T. Outcomes of extracapsular surgery in eye camps of eastern Nepal. Br J Ophthalmol 2001; 85: 648-52.
3.Chang DF. Tackling the greatest challenge in cataract surgery. Br J Ophthalmol 2005; 89: 1073-4.
4.Vogel A, Capon MR, Asiyo-Vogel MN, Eginald Birngruber R. Intraocular photodisruption with picosecond and nanosecond laser pulses: tissue effects in cornea, lens, and retina. Invest Ophthalmol Vis Sci 1994; 35: 3032-44.
5.Durham DG, Gills JP. Three thousand YAG lasers in posterior capsulotomies: an analysis of complications and comparison to polishing and surgical decisions. Trans Am Ophthalmal Soc 1985; 83: 218-35.
6.Terry AC, Stark WJ, Newsome DA, Maumenee AE, Pina E. Tissue toxicity of laser damaged intraocular lens implants. Ophthalmology 1985; 92: 414-8.
7.Terry AC, Stark WJ, Maumenee AE, Fagadau W .Neodymium-YAG laser for posterior capsulotomy. Am J Ophthalmol 1983; 96: 716-20.
8.Flohr MJ, Robin AL, Kelley JS. Early complications following Q switched neodymiumYAG laser posterior capsulotomy. Ophthalmology 1985; 92: 360-9.
9.Steinnert RF, Cionni RJ, Osher RH, Blumenkranz MS, Koch DD, Novak KD, et al. Complications of Cataract Surgery. In: Albert DM, Jakobiec FA. Principles and Practice of Ophthalmology: Clinical Practice. Philadelphia: WB Sunders, 2000; pp 1551-98.
10.Rosenfeld PJ. Intravitreal avastin: the low cost alternative to lucentis? Am J Ophthalmol 2006; 142: 141-3.
11.Aslam TM, Patton N. Methods of assessment of patients for Nd:YAG laser capsulotomy that correlate with final visual improvement. BMC Ophthalmol 2004; 4: 1-6.
12.Schaumberg D, Dana MR, Christen WG, Glynn RJ. A systematic overview of the incidence of posterior capsule opacification. Ophthalmology 1998; 105: 1213-21.
13.Ambler JS, Constable IJ. Retinal detachment following Nd:YAG capsulotomy. Aust N Z J Ophthalmol 1988; 16: 337-41.
14.Ranta P, Tommila P, Kivela T. Retinal breaks and detachment after neodymium. YAG laser posterior capsulotomy: five-year incidence in a prospective cohort. J Cataract Refract Surg 2004; 30: 58-66.
15.Léonard PA, Klevering BJ, de Keizer RJ. Complications of secondary surgical capsulotomy in pseudophakic and aphakic eyes. Ophthalmic Surg 1992; 23: 330-5.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: