
Khalid Maudood Siddiqui ( Department of Anaesthesia and Intensive Care, Aga Khan University, Karachi. )
Sobia Khan ( Department of Anaesthesia and Intensive Care, Aga Khan University, Karachi. )
June 2010, Volume 60, Issue 6
Case Reports
Abstract
Epidermolysis bullosa is a group of inherited disorders characterized by blistering of the skin as a result of minor trauma. We managed an infant with epidermolysis bullosa undergoing inguinal hernia repair. Anaesthesia was induced with oxygen/nitrous oxide mixture and sevoflurane. Oral tracheal intubation was done with a lubricated laryngoscope blade with KY jelly using atracurium 0.5mg/kg and fentanyl 0.1µgm/kg. To avoid frictions on the skin, endotracheal tube was tied with ribbon gauze and fixed around the neck. Pulse-oximetry probe and electrocardiogram electrodes were placed, and then attached to the patient\'s skin covered with KY jelly. Peripheral venous access was secured in the right foot and sutured. These methods were effective to avoid new blisters and useful for infant safety.
Case History
A 3 month old child with congenital epidermolysis bullosa was admitted with the complaint of reducible swelling in right scrotum since two months, vomiting on and off since one month and fever at presentation. On his past history he was born full term via normal vaginal delivery, his birth weight was 3.4 kg. He had no vaccination except oral polio vaccine (OPV) because he had rashes and denuded skin all over the body. On his family history his paternal aunt had a baby boy with epidermolysis bullosa who died at 33 days after birth.
General and physical examination, showed pallor and rashes all over the body. His cardiovascular and respiratory systems were unremarkable. Abdomen was soft, with no distension or visceromegaly. A reducible swelling was found in his right scrotum.
Baby\'s preoperative evaluation showed a heart rate 130/min, respiratory rate 30/min and temperature 39°C. His blood culture and sensitivity report were positive for pseudomonas. Since the child was severely anaemic and septic, he was transfused packed red cells and started on intravenous antibiotics. The baby was stabilized within 5 days and then his right inguinal hernia was planned.
Anaesthetic Management:
In operating room the baby was very gently taken care of and minimum handling was ensured Intravenous line was already established in foot with 24 G cannula. ECG electrodes were applied taking care not to use denuded skin, extra gel applied to ECG electrodes to ensure extra protection of denuded skin. Non-Invasive Blood Pressure (NIBP) was not applied at all as both upper limbs had severe rashes. SPO2 probe was applied in foot (Figure).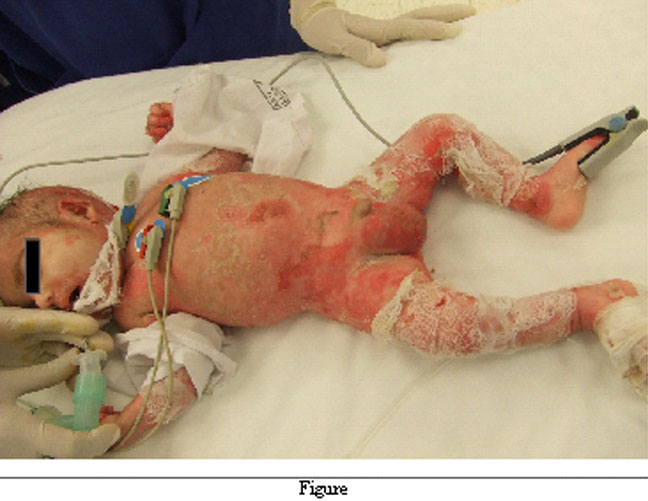
The baby was given general anaesthesia. He was induced with sevoflorane. After achieving adequate Minimal Alveolar Concentration (MAC) injection atracuriam 0.5mg/kg was given and gentle laryngoscopy was done and ETT size 3 was inserted in trachea after generous lubrication. The tube was fixed at 10 cm with ribbon gauze instead of tapes. The patient was ventilated in controlled mode via T piece (Manual ventilation). Intravenous fentanyl 5 µgm was given as analgesia. Since caudal block and paracetamol suppository both were not possible, a right inguinal block was done at the end of surgery. The baby had uneventful anaesthesia and was extubated successfully. He was shifted to the ward after routine postoperative course in recovery room.
Discussion
Epidermolysis bullosa (EB) is a heterogenous group of mechanobullous disorders characterized by painful blister formation as a result of minor trauma to the skin. This disease can involve the skin, mucosae, and internal organs. It is an inherited disease, with the exception of the acquisita type. Inherited epidermolysis bullosa has been grouped in three major types according to the level of the blister formation: simplex, junctional, or dystrophic. It has been subgrouped based on ultrastructural level of splitting and gene/protein defects and more than 23 subtypes have been documented.1
Epidermolysis bullosa simplex varies from mild blistering limited to the hands and feet to severe form with generalized blistering and involvement of mucous membranes and nails. It is usually nonscarring, unless secondary infection occurs. Inheritance is autosomal dominant. Pathophysiology is related to mutations in the genes that encode Keratins 5 and 14. These keratins make up part of the scaffolding that anchors basal keratinocytes to the basement membrane. Structural abnormalities lead to separation of the basal cells from the basal membrane when the skin is exposed to friction, trauma, or heat.
Junctional epidermolysis bullosa varies from mild to severe (Herlitz, letalis) types. Transmission is autosomal recessive. The disease usually presents with generalized blistering and heals with atrophic scars. Most patients with junctional EB die early. Survivors may have severe dental enamel dysplasia and anaemia. Mutations may occur in the genes encoding Laminin2 a component of anchoring fibrils that keep the epidermis bound to the dermis. Several variants are recognized. Now correction of junctional epidermolysis bullosa by transplantation of genetically modified epidermal stem cells has evolved which has been quite successful.3
Dystrophic epidermolysis bullosa varies from a mild autosomal dominant form with lesions on hands, knees, and elbows to severe autosomal recessive form with generalized blistering, growth retardation, anaemia, mucosal blistering, tremendous disability, and deformity. Healing of blisters leaves residual scars and milia. Digital fusions and contractures occur with the formation of mitten deformities of the hands and feet. All forms are related to mutations in type VII collagen, which compromises the anchoring fibrils that hold the epidermis and dermis together.
Patients with epidermolysis bullosa usually come to operating room for wound dressing. Anaesthetic technique could be general or regional or both.4 Regional technique is recommended only as a precise indication. General rule for management is "no touch" principle. Adhesive dressing should never be used. Extra care is needed during positioning.
Sedative premedication is helpful in children to avoid restlessness and prevent injury during inhalational induction. To prevent excessive salivation atropine or glycopyrolate are also used. Minimal monitoring is advisable.5 Pulse oximeter probes are difficult to place in certain cases but it can be used safely to monitor oxygen saturation. Electrocardiogram monitoring is difficult but can be done by simply removing the adhesive pads of electrodes.6 The choice of induction of anaesthesia is preferably intravenous. Gentle care is required when using the face mask and must be prepared by several layers of Vaseline gauze. Lubricated oral airways can be used with care. Laryngoscopes blades should be well lubricated with water soluble gel and tracheal tube should be well lubricated, under sized and uncuffed. In several trials there was no major tracheal complication from airway management or intubation.7,8 Narcotics or non steroidal anti inflammatory drugs are safe for analgesia.9 Regional anaesthesia in combination with general anaesthesia is also useful for intra and post operative pain control. Epidural anaesthesia in epidermolysis bullosa cases has been also reported.10
Conclusion
Anaesthetizing an infant with Epidermolysis Bullosa is a challenge as both skin and mucous membranes are affected by rashes and denudation making all procedures very difficult because of application of monitors, establishing intravenous lines and laryngoscopy. These types of cases should be done in specialist centres. Extra care is required to minimize the further trauma.
References
1.Fine JD, Johnson LB, Wright JT. Inherited blistering diseases of the skin. Pediatrician 1991; 18: 175-87.
2.Carter D, Lin A, Varghese M, Caldwell N, Pratt L, Eisinger M. Treatment of junctional epidermolysis bullosa with epidermal autografts. J Am Acad Dermatol 1987; 17: 246-50.
3.Mavilio F, Pellegrini G, Ferrari S, Di Nunzio F, DiLorio E, Recchia A, et al. Correction of junctional epidermolysis bullosa by transplantation of geniticaly modified epidermal stem cells. Nat Med 2006; 12: 1397-402.
4.Chevaleraud E, Ragot JM, Glicenstein J. (Anesthesia for hand surgery in patients with epidermolysis bullosa). Ann Chir Main Memb Super 1995: 14: 296-303.
5.Association of Anaesthetists of Great Britain and Ireland. Recommendations for Standards of Monitoring during Anaesthesia and Recovery. London: Association of Anaesthetists of Great Britain and Irelaand, 1988.
6.Holzman RS, Worthen M, Johnson KL. Anaesthesia for children with junctional epidermolysis bullosa (letalis). Can J Anaesth 1987; 34: 395-9.
7.Iohom G, Lyons B. Anaesthesia for children with epidermolysis bullosa: a review of 20 year experience. Eur J Anaesthesiol 2001; 18: 745-54.
8.Herod J, Denyer JR, Goldman A, Howard R. Epidermolysis bullosa in children: Pathophysiology, anaesthesia and pain management. Paediat Anaesth 2002; 12: 388-97.
9.Hagen R, Langenberg C. Anesthetic management in patients with epidermolysis bullosa dystrophica. Anaesthesia 1988; 43: 482-5.
10.Doi S, Horimoto Y. Subcutaneous tunneling of an epidural catheter in a child with epidermolysis bullosa. Acta Anaesthesiologica Scandinavia 2005; 50: 394-5.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: