
Ayaz Hussain Shaikh ( Department of Cardiology, Tabba Heart Institute, Karachi. )
Bashir Hanif ( Department of Cardiology, Tabba Heart Institute, Karachi. )
Amina Adil ( Department of Cardiology, Tabba Heart Institute, Karachi. )
Sharukh Hashimi ( Department of Cardiology, Tabba Heart Institute, Karachi. )
Hammad Ali Qazi ( Department of Cardiology, Tabba Heart Institute, Karachi. )
Iqbal Mujtaba ( Department of Cardiology, Tabba Heart Institute, Karachi. )
May 2010, Volume 60, Issue 5
Original Article
Abstract
Objective: To determine the doppler derived mean gradients of St Jude mechanical prosthesis in early postoperative period in patients undergoing valve replacement at a tertiary care cardiac centre.
Methods: Medical records of 190 consecutive patients who underwent 233 mitral, aortic or dual (mitral and aortic) valve replacement by St Jude bileaflet mechanical prosthesis at Tabba Heart Institute, between March 2006 to December 2008 were reviewed. Doppler derived mean gradients were assessed predischarge and recorded.
Results: There were 98 (51.5%) males and 92 (48.5%) females in the study cohort. The mean age was 40 ± 14 years. Of the total, 101 (53%) had mitral, 46 (24.2%) had aortic and 43 (22.6%) patients had dual valve replacement. Doppler derived mean gradient was assessed across 144 mitral and 89 aortic St Jude mechanical prosthesis. Doppler derived mean gradient for St Jude mitral prosthesis was 3.5 mm Hg and for St Jude aortic prosthesis was 10.2 mm Hg.
Conclusions: The study determines baseline gradients across mitral and aortic St Jude mechanical prosthesis in our population. These can be used as reference gradients to assess St Jude prosthetic valve function in patients who did not have early postoperative doppler assessment (JPMA 60:374; 2010).
Introduction
Valve replacement with prosthetic valves (mechanical or bioprosthetic) is the only viable option for severely diseased native valves particularly those of rheumatic origin. Prosthetic valve surgery entails a life long commitment from both the patient and the cardiologist. Without regular follow-up including long-term prosthetic haemodynamic assessment, catastrophic complications can occur. It is important to obtain accurate records of prosthetic valve function after valve replacement surgery.1 The early postoperative echocardiogram should be used to document the stability of the valve, the presence and extent of valvular or paravalvular regurgitation, and the transvalvular pressure gradients.2
Noninvasive methods such as fluoroscopy, M-mode and two-dimensional echocardiography have been used for this purpose but these methods have significant limitations.3 Cardiac catheterization has been reliable for definite identification of prosthetic valve malfunction, but this procedure also has associated risks.1 A more sensitive noninvasive tool, doppler echocardiography was first used for evaluation of prosthetic valve function in 1983 and is now a well-established method for assessment of prosthetic valve function.4
Due to limited visualization of prosthetic valve on 2D imaging because of artifacts, doppler assessment of valve is essential. Out of all doppler derived parameters, mean gradient is being considered as most important marker for assessment of prosthetic valve function. It is very important to document patient\'s baseline mean gradient in early postoperative period because these gradients can be used in future detection of prosthesis malfunction.5
Emerson et al studied mean gradient in 180 St Jude mechanical aortic prosthesis and found mean gradient of 14±5 mm Hg.6 Bitar and colleagues found doppler-derived mean gradient average 4 ± 2 mm Hg for mitral St Jude mechanical prosthesis.7 These values serve as a reference reading in case an initial post operative doppler assessment was not made in a patient with suspected prosthesis dysfunction.
Unfortunately the routine assessment of postoperative doppler derived prosthetic valve gradients has been underutilized in our population. No data was found after robust literature search addressing the mean doppler gradients in patients undergoing valve replacement with St Jude mechanical prosthesis in our population. The aim of our study was to determine the early postoperative mean gradients for mitral and aortic St Jude mechanical prosthesis which is the most widely used mechanical prosthesis in current clinical practice. These gradients can be utilized as reference gradients for our population.
Patient and Methods
Medical records of 190 consecutive patients who underwent 233 mitral, aortic or dual (mitral and aortic) valve replacement by St Jude mechanical prosthesis at Tabba heart institute between March 2006 to December 2008 were reviewed. All patients of either gender and of any age who underwent mitral, aortic or dual (mitral and aortic) valve replacement with St Jude mechanical prosthesis were included. Patients who had undergone placement of bioprosthetic valve and those with re-operation due to prior prosthesis malfunction (infective endocarditis, valve thrombosis) were excluded.
Echocardiographic studies were performed with specific systems (SIEMENS Accuson CV 70) by using 2.5- MHz independent transducer by board certified experienced staff cardiologists.
Doppler velocity profiles across the St. Jude Medical valves at mitral and aortic location were obtained on 7th day (mean) from left parasternal, apical, suprasternal, and right parastemal positions with an attempt to place the ultrasound beam directly perpendicular to the prosthetic valve plane. Doppler sample volume placement was aided by two-dimensional echocardiographic imaging. Subsequently mean gradient was derived by tracing the maximally obtained velocity enveloped from at least 5 sample volumes and taking their mean as a representative mean gradient.
A performa was designed to collect information including, age, gender, history of co-morbids like diabetes (defined as a fasting glucose > 126 mg/dl or on treatment), hyperlipidaemia (fasting cholesterol > 200 mg/dl or on treatment), hypertension (systolic blood pressure > 140/90 mmHg or on treatment) and smoking. Left ventricular function was visually estimated by transthoracic echocardiogram. Etiology of valve disease was also recorded.
The data was also collected about St Jude mechanical prosthesis location i.e. mitral, aortic or dual valve (mitral and aortic), valve size and doppler derived mean gradients across St Jude mechanical prosthesis.
All the variables were entered into the Statistical Package for Social Sciences software, version. 15. (SPSS Inc) for data analysis. Descriptive statistics were computed and presented as means and standard deviations were calculated for continuous variables like age, LVEF and gradients of St. Jude prosthesis. Frequencies and percentages were computed for gender, diabetes, hypertension, dyslipidaemia, location and sizes of St. Jude prosthesis.
Results
Total of 190 patients were included in this study. Table-1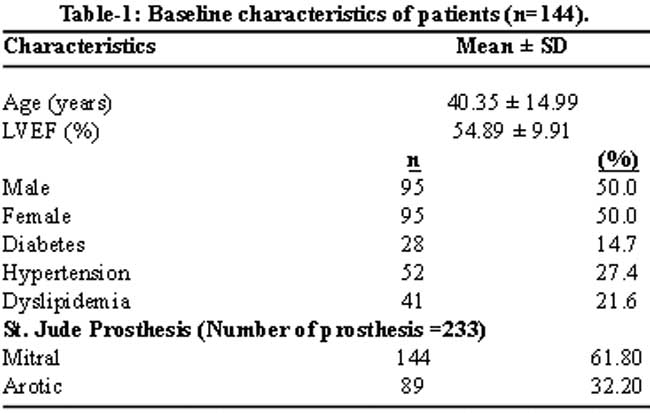
shows the baseline demographic and clinical characteristics of the studied cohort. There were 98 (51.5%) males and 92 (48.5%) females in the study. The mean age was 40 ± 14 years.
Of the total, 101 (53%) patients had mitral, 46 (24.2%) had aortic and 43 (22.6%) had dual valve replacement with St Jude mechanical prosthesis. Most common underlying disease was rheumatic heart disease (77.9%). Most commonly used mitral size was 27 (37.5%) and most commonly used aortic size was 21 (48.3%). Distribution of valve sizes are shown in Table-2.
Doppler derived mean gradient was assessed across 144 mitral and 89 aortic St Jude mechanical prosthesis. Doppler derived mean gradient for St Jude mitral prosthesis was 3.83 ± 0.81 mm Hg and for St Jude aortic prosthesis was 11.72 ± 1.24 mm Hg. Mean doppler gradients for different prosthetic valve sizes were also calculated, shown in Table-3.
Discussion
Assessment of prosthetic valve function is a commonly encountered question in practice of clinical cardiology. The number of patients undergoing valve replacement due to significant burden of rheumatic valvular heart disease is increasing. Mechanical valve acts as a double edged sword. It provides durable solution for valvular dysfunction but on the other hand has potential risks related to anticoagulation and valve dysfunction i.e. infective endocarditis, valve thrombosis, pannus formation and dehiscence.
It is recommended to record baseline prosthetic valve function, including mean gradients after surgery prior to discharge. Because of its feasibility and sensitivity, Doppler echocardiography has gained popularity as the method of choice for serial evaluation of prosthetic valve function. Doppler derived mean gradient across prosthesis not only provides baseline information but is invaluable for future assessment of prosthesis dysfunction. The St. Jude Medical valve has excellent haemodynamic performance and reliability and is currently the most frequently implanted prosthetic valve.7
Mean doppler gradients for St Jude mechanical prosthesis at mitral and aortic location have been previously described.8 Mean gradients were reported in five patient groups who had St Jude mechanical prosthesis at aortic location. According to valve sizes of 19 mm, 21 mm, 23 mm, 25 mm, and 27 mm, mean gradients were 16 ± 6, 16 ± 6, 14 ± 5, 12 ± 5, and 12 ± 6 mm Hg respectively. Differences in gradients among the five valve sizes were not statistically significant (p < 0.05).6
Miller and colleagues found mean gradient of 14.4 ± 7 mm Hg across 44 St Jude aortic prosthesis.9
In our study commonly implanted St Jude aortic prosthesis sizes were 19mm, 21mm, 23mm and 25mm. Mean doppler derived gradients were 12.79 ± 0.89, 11.8 ± 0.98, 11.36 ± 1.28 and 11.06 ± 1.2 mm Hg respectively with average mean gradient value of 11.72 ± 1.24 mm Hg.
Mean gradients were reported in four patient groups who had mechanical St jude prosthesis at mitral location. According to valve sizes of 25 mm, 27 mm, 29 mm and 31 mm, mean gradients were 3 ± 1, 5 ± 2, 4 ± 2, and 4 ± 2 mm Hg respectively.10
Lengly and colleagues found mean gradient of 4±1mm Hg across 66 mechanical St Jude mitral prosthesis.11
Our study\'s commonly implanted St Jude mitral prosthesis sizes were 25mm, 27mm, 29mm and 31mm. Mean doppler derived gradients were 4.5 ± 0.83, 3.81 ± 0.75, 3.65 ± 0.69 and 3.50 ± 0.76 mm Hg respectively with average mean gradient value of 3.83 ± 0.81mm Hg.
To our knowledge, this is the first study from Pakistan which has looked at the most commonly used mechanical valve with Doppler derived mean gradients across all possible valve sizes. Early postoperative measurement of doppler mean gradient is of pivotal importance in future assessment of prosthesis dysfunction and is invaluable in clinical decision making.12
We strongly recommend measurement of mean gradients across prosthetic valve in early postoperative period which can be used as baseline value for future reference. Unfortunately this practice is not being done judiciously. The study determined baseline gradients across mitral and aortic St Jude mechanical prosthesis in our population. This can be used as reference gradients to assess mitral and aortic St Jude mechanical prosthetic valve function in patients in whom early postoperative doppler assessment was not performed.
References
1.Burstow DJ, Nishimura RA, Bailey KR, Reeder GS, Holmes DR Jr, Seward JB, et al. Continuous wave Doppler echocardiographic measurement of prosthetic valve gradients. A simultaneous Doppler-catheter correlative study. Circulation 1989; 80: 504-14.
2.Reisner SA, Meltzer RS. Normal values of prosthetic valve Doppler echocardiographic parameters: A review. J Am Soc Echocardiogr 1988; 1: 201-10.
3.Mintz GS, Carlson EB, Kotler MN. Comparison of noninvasive techniques in evaluation of the nontissue cardiac valve prosthesis. Am J Cardiol 1982; 49: 39-44.
4.Alam M, Rosman HS, Lakier JB, Kemp 5, Khaja F, Hautamaki K, et al. Doppler and echocardiographic features of normal and dysfunctioning bioprosthetic valves. J Am Coll Cardiol 1987; 10: 851-8.
5.Panidis IP, Ross J, Mintz GS. Normal and abnormal prosthetic valve function as assessed by Doppler echocardiography. J Am Coll Cardiol 1986; 8: 317-26.
6.Perin E, Jin BS, de Castro CM, Ferguson JJ, Hall RJ. Doppler echocardiography in 180 normally functioning St. Jude Medical aortic valve prostheses. Early and late postoperative assessments. Chest 1991; 100: 988-90.
7.Bitar JN, Lechin ME, Salazar G, Zoghbi WA. Doppler echocardiographic assessment with the continuity equation of St. Jude Medical mechanical prostheses in the mitral valve position. Am J Cardiol 1995; 76: 287-93.
8.Milano AD, De Carlo M, Mecozzi G, D\'Alfonso A, Scioti G, Nardi C, et al. Clinical outcome in patients with 19-mm and 21-mm St. Jude aortic prostheses: comparison at long-term follow-up. Ann Thorac Surg 2002; 73: 37-43.
9.Miller FA Jr, Callahan JA, Taylor CL, Larson-Keller JJ, Seward JB. Normal aortic valve prosthesis haemodynamics: 609 prospective Doppler examinations. Circulation 1989; 80: II-169.
10.Rosenhek R, Binder T, Maurer G, Baumgartner H. Normal values for Doppler echocardiographic assessment of heart valve prostheses. J Am Soc Echocardiogr 2003; 16: 1116-27.
11.Lengley M, Miller FA Jr, Taylor CL, Larson-Kellar JJ, Seward JB, Tajik AJ. Doppler hemodynamic profile of 456 clinically and echo-normal mitral valve prosthesis Circulation 1990; 82 III-43.
12.Mahdhaoui A, Majdoub MA, Bouraoui H, Ernez Hajri S, Jeridi G, Trimeche B, et al. [Evaluation of the hemodynamic profile of mitral Saint Jude Medical prostheses in the early and late postoperative period]. Arch Mal Coeur Vaiss 2003; 96: 977-83.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: